
Interdisciplinary Orthodontic and Surgical Management of Class III Malocclusion in Adult Patients
Abstract
The treatment of class III malocclusion differs depending on the age of the patient. In adult patients, alternatives include either orthodontic dentoalveolar compensation treatment or a combined ortho-surgical approach. The aim of this paper is to present the orthodontic and surgical treatment of a 24 year old adult patient with increased anterior face height, a class III skeletal pattern and mandibular asymetry. Previous orthodontic treatment with removable appliances obtained a 1 mm overbite and overjet. Intraorally, class III molar relationship was observed, proclined upper incisors, retroclined lower incisors and a deviated lower midline. The main complaint was facial esthetics which required surgical intevention. After pre-surgical orthodontic preparation the maxilla was repositioned by a Le Fort I osteotomy and the mandible was set back using the Obwegeser-Dal Pont method. Final assesment revealed both functional and esthetic dentofacial results. A combination of orthodontic treatment and orthognathic surgery is often required in adult patients with dental malocclusion and skeletal discrepancies.
Author Contributions
Academic Editor: Vinayak Raghunathan, Assistant Professor, India.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Camelia Szuhanek, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Class III malocclusion is a challenge to the orthodontic profession representing a complex skeletal imbalance between upper and lower jaw growth patterns accompanied by various dentoalveolar and soft tissue compensations.1 Given the complexity of the malocclusion three treatment options are available: growth modification, orthodontic camouflage and surgical treatment. Timing of growth modification treatment is important and can only take place before the pubertal growth spurt.2 Thus for adult patients, two alternatives remain: dentoalveolar compensation or a combination of orthodontic treatment and orthognathic surgery. When facial esthetics are compromised, orthodontic treatment might not be enough to meet the complaints of the patient. In order to provide esthetic, functional and stable results, the orthodontist and the surgeon must collaborate during the diagnosis stage so that a detailed treatment plan for the patient is reached. 3
Class III are mainly characterized by sagital skeletal discrepancies: mandibular prognathism, maxillary retrognathism or both.3, 4 Dental discrepancies include class III Angle molar relation and anterior crossbite, often with an increased negative overjet. The specific facial profile of the patient is prognathic, with a proeminent chin, which is considered both an esthetic and psychological problem and is a major reason why many adult patients choose a surgical correction. 4, 5, 6
The treatment of class III malocclusion differs depending on the age of the patient and on the severity of the skeletal and dental discrepancies.3, 4, 6, 7Orthodontic dentoalveolar compensation or orthodontic camouflage involves obtaining an acceptable result by proclining the maxillary incisors and retroclining the mandibular incisors. This is recommended in mild dento-skeletal dicrepancies when the mandibular incisors are proclined. 8
In severe class III cases, with large skeletal and dental discrepancies, surgery is recommended in order to improve occlusion and facial esthetics. The surgical treatment plan is mainly based on the correction of the antro-posterior dicrepancy and includes repositioning of the jaws in the sagittal plane: either mandibular retrusion, maxillary protrusion, or both, depending on the case. Bimaxillary surgery is recommended in severe sagittal discrepancies, where the problem cannot be corrected by single-jaw surgery 3, 9, 10. Authors have reported general limits of 6-8 mm for maxillary advancement and 4-6 mm for mandibular setback. 9
Le Fort I osteotomy is a surgical procedure that involves repositioning of the maxilla and allows modifications in all three planes, being mostly recommended in maxillary hypoplasia 11, 12. Sagittal ramus split osteotomy was introduced by Obwegeser and later modified by Le Pont, and is recommended inprognathic mandible set back procedures.13
The aim of this paper is to present the orthodontic and surgical treatment of a 24 year old adult patient with increased anterior face height, a class III skeletal pattern and mandibular asymetry.
Case Report
A 24-year old patient presented to a private clinic with the chief complaint of poor facial estheticsassociated with a protruded mandible and chin. Patient history revealed a class III pattern in the family on the side of the father and previous orthodontic intervention during childhood, with a removable appliance to correct the anterior crossbite.
Orthodontic examination digital photographs were taken before the patient underwent the initial cinical examination. Frontal esthetic analysis revealed a long face, an increased third floor of the face and an asymmetry due to mandibular deviation to the left. Lateral view analysis disclosed a concave profile, with a deficient nasomaxillary area and proeminent chin. The lower lip was protruded, the upper lip was retruded and the mentolabial anlge was reduced. (Figure 1)
Figure 1.Initial extraoral photographs
Intraoral examination revealed bilateral Angle’s class III molar relationship, class III canine relationship on the right and class I on the left, a deviated lower dental midline to the left of the patient, a visible negative tip in the right upper lateral incisor and canine, crossbite between 1.2. and 4.3 and 4.4, retroclined lower incisors, proclined upper incisors, with a 1 mm overbite and overjet . (Figure 2)
Figure 2.Initial intraoral photographs
The panoramic radiograph examination showed impacted bilateral mandibular third molars, and one maxillary third molar.Cephalometric analysis disclosed a skeletal class III (ANB -5 degrees), with a retruded maxilla and a protruded mandible (SNA 78 degrees and SNB 83 degrees). The patient is a hyperdivergent type, with FMA 30 degrees and IMPA 77 degrees, which suggests retruded lower incisors. Examination of soft tissue on the profile radiograph shows a concave profile and a protruded lower lip. (Figure 3).
Figure 3.Initial panoramic and lateral cephalometric radiographs
Primary treatment objectives were to improve facial esthetics and correct the protruding chin and concave soft tissue profile. Other treatment objectives were to obtain a functional occlusion with class I molar and canine relationships, correct the lower midline deviation and retroclination of lower incisors.
Firststage of treatment began with third molar odontectomies. Afterwards the patient was bonded with conventional straight-wire metallic orthodontic braces with an0.22’’ Roth slot.For patient confort the upper arch was bonded first, bonding of the lower arch following a month later. The archwire sequence was as follows: 0.012”, 0.014”, 0.016” NiTi archwires progressing to 0.016 × 0.016”, 0.016 × 0.022” and 0.019x0.025 NiTi archwires, ending with a 0.019x0.025 SS archwires.
The pre-surgical orthodontic preparation successfully met the following objectives: levelling and aligning, flattening of curbe of Spee, proclination of the lower incisors and elimination of dental compensations. Before surgery, the patient had a normal position of the lower incisors, with IMPA 88 degrees. (Figure 4) Before surgery, a slight anterior open bite and an anterior crossbite could be observed, due to the elimination of dental compensations. Crimpable hooks were placed between each tooth on the 0.019x0.025 SS archwires, to allow placement of intermaxillary elastics after surgery. (Figure 5).
Figure 4.Pre-surgical extraoral photographs, after orthodontic preparation and preoperative lateral cephalometric radiograph
Figure 5.Pre-surgical intraoral photographs
The surgical treatment included Le Fort I osteotomy for impactation and anterior traction of the maxilla. The Obwegeser-Dal Pont method for the set back of the mandible was used. The surgical and post-surgical phase had no complications.
Post-surgical orthodontic treatment was started 4 weeks after the surgery. Wearing of bilateral box elastics was recommended in order to improve interdigitation. (Figure 6) The orthodontic treatment was finished on 0.019x0.025 SS archwires. Post-surgery cephalometric analysis revealed an increase in SNA value by 4 degrees (SNA 82 degrees) and a decrease in SNB value also by 4 degrees (SNB 79 degrees). The patient was now in a skeletal class I, with ANB 3 degrees. An examination of the soft tissue on the radiograph reveales a better relation between the upper and lower lip. (Figure 7).
Figure 6.Post-surgical intraoral photographs, with bilateral box elastics
Figure 7.Post-surgical panoramic and lateral cephalometric radiograph.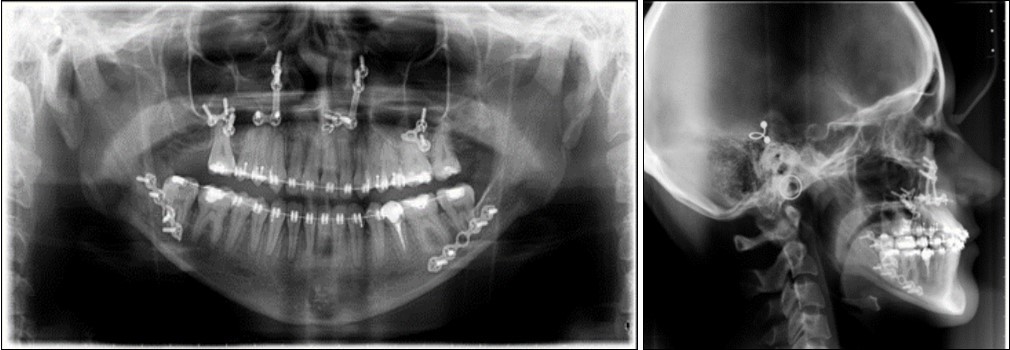
Results
Post-treatment extraoral examination revealed that all pretreatment objectives were met. The arches were leveled and aligned, obtaining a stable occlusion with both canine and molar class I relationships. Lower incisors mainteined a normal position at the moment of debonding.
Both the mandibular deviation and the dental midline were corrected improving facial esthetics and dental occlusion. The profile of the patient dramatically improved from concave to straight, the new skeletal ralation providing better support for the upper and lower lips with no lip strain..
The total duration of the treatment was 24 months. The patient was fitted with vacuum formed retainers for the upper and lower arches and a bonded retainer from cuspid to cuspid in the lower arch. The patient was satisfied with facial esthetics, chin projection, facial profile and smile. (Figure 8), (Figure 9).
Figure 8.Post-treatment extraoral photographs
Figure 9.Post-treatment intraoral photographs
Discussion
Class III malocclusions often imply a growth deficit in the maxilla and a more anterior growth in the mandible. According to Silva et al., prevalence of class III patients in European populations varies from 2% to 6%.14 This kind of anomaly is accentuated in hypodivergent growth patterns, while the hyperdivergent growth pattern tends to minimise it, provided that the vertical excess (facial height) does not become a problem.15
Treatment in such cases remains a challenge for the orthodontic specialists, especially in borderline cases when a decision between camouflage and surgical treatment should be made. Studies show that Wits appraisal is a decisive indicator determining either the orthodontic camouflage or orthognathic treatment of class III patients, together with the IMPA angle and the interincisal angle. 16, 17
Early orthodontic treatment following a correct diagnosis can reduce the severity of a class III malocclusion in adulthood. Thus children with developing class III should be evaluated regarding family history of class III, functional mandibular shift, dental relationships and jaw discrepancies. 15 Still, surgical class III correction treatment is widely accepted among non-growing patients, including cases where camouflage treatments are possible, mainly because facial esthetics is a main concern which orthodontic treatment can not solve alone.18
The use of digital patient records such as x-rays and digital photos, is particularly useful in cases where patients are treated in interdisciplinary teams.19 In the present case report, collaboration between orthodontic and surgical treatment was a success, with excellent esthetic and functional results. From a skeletal class III (ANB –5 degrees), the increase in ANB angle value was 8 degrees after the bimaxillary surgery, final ANB angle value being 3 degrees and a class I skeletal class.
In Class III cases orthodontic-surgical cases, the pre-surgical orthodontic stage is necessary to correct dental compensations that could cause interferences during the surgical repositioning of the maxilla and mandible 8. In this case, it was achieved with Roth prescription and a normal sequence of archwires.
Conclusion
Interdisciplinary management of Class III malocclusions with orthodontic-surgical treatment can have excellent results, leading to a functional occlusion and improved facial esthetics.
The importance of a good diagnosis and treatment plan is as relevant and necessary as the communication between orthodontist and surgeon, in such complex cases.
References
- 1.Mackay F, Jones J A, Thompson R, Simpson W. (1992) Craniofacial form in class III cases,”. , British Journal of Orthodontics 19(1), 15-20.
- 2.Rabie B, R W Wong, G U Min. (2008) Treatment in borderline class III malocclusion: orthodontic camouflage (extraction) versus orthognathic surgery,”. , The Open Dentistry Journal 2, 38-48.
- 3.Furquim B A, De Freitas KMS, Janson G.Class III Malocclusion Surgical-Orthodontic Treatment. Case reports in dentistry.;2014: 868390.; PMCID:. 4241289.
- 4.LS1 Stojanović, Mileusnić I, Mileusnić B. (2013) Cutović T Orthodontic-surgical treatment of the skeletal class III malocclusion: a case report, Vojnosanit Pregl. 70(2), 215-20.
- 5.Kongo E. (2018) Treatment of Maxillary Retrusion-Face Mask with or without RPE?. , Balk J Dent Med, Vol 22.
- 6.García-López E Huízar-GonzálezI, Ramírez-Aguilar M Orozco-PartidaJ. (2017) Orthodontic surgical management of a skeletal class III patient with laterognathia,RevistaMexicana deOrtodoncia,5(2):. 95-101.
- 7.Mojica N, Gómez I. (2018) Surgical-orthodontic treatment of a class III patient with asymmetry due to mandibular deviation. Case report. , Revista Mexicana de Ortodoncia 6(1), 50-5.
- 8.PatelK KauC. (2017) WaiteP, CelebiA- The surgical management of skeletal disproportion with lingual orthodontics and three-dimensional planning, Ann Maxillofac Surg. 7, 112-6.
- 9.HaryaniJ NagarA. (2016) MehrotraD, RanabhattR- Management of severe skeletal Class III malocclusion with bimaxillary orthognathic surgery,ContempClin Dent. , Oct-Dec; 7(4), 574-578.
- 10.M S Ravi, Shetty NillanK, Rajendra B Prasad-. (2012) Orthodontics-surgical combination therapy for Class III skeletal malocclusion,ContempClin Dent. , Jan-Mar; 3(1), 78-82.
- 11.Togawaa R, Iinob S, Miyawakic S. (2010) Skeletal Class III and open bite treated with bilateral sagittal split osteotomy and molar intrusion using titanium screws. , Angle Orthodontist 80(6).
- 12.Edward P Buchanan, Charles H Hyman, BA- LeFort I. (2013) . , Osteotomy Semin Plast Surg. Aug; 27(3), 149-154.
- 13.BöckmannR MeynsJ, DikE KesslerP. (2014) The Modifications of the Sagittal Ramus Split Osteotomy: A Literature Review,PlastReconstrSurgGlob Open. 2(12), 271.
- 14.Silva R G, Kang D S. (2001) Prevalence of malocclusion among Latino adolescents. , Am JOrthodDentofacialOrthop 119(3), 313-315.
- 15.Chaudhari PK ZereE, Sharan J, Dhingra K, Tiwari N. (2018) Developing Class III malocclusions: challenges and solutions,Clinical. , Cosmetic and Investigational Dentistry 10, 99-116.
- 16.Martinez P, Bellot-Arcis C, Llamas J M, Cibrian R, Gandia J L et al. (2017) Orthodontic camouflage versus orthognathic surgery for class III deformity: comparative cephalometric analysis. , Int J Oral Maxillofac Surg 46, 490-495.
- 17.Stellzig-Eisenhauer A, Lux C J, Schuster G. (2002) Treatment decision in adult patients with class III malocclusion: orthodontic therapy or orthognathic surgery?. , Am J Orthod Dentofac Orthop 122, 27-37.
Cited by (1)
- 1.Alogaibi Yahya A., Alsulaimani Fahad F., Jamal Basem, Mitwally Rania, Scribante Andrea, 2021, Combined Orthodontic and Surgical Management for Treatment of Severe Class III Malocclusion with Anterior and Posterior Crossbites, Case Reports in Dentistry, 2021(), 1, 10.1155/2021/5579077