
Non-Syndromic Multiple Keratocystic Odontogenic Tumor: A Case Report
Abstract
A Keratocystic Odontogenic Tumor (KCOT) is a benign odontogenic lesion that is well-known for its histopathological features and invasive clinical behaviors. KCOTs may be non-syndromic or syndromic, and the syndromic type presents a higher risk of recurrence and invasive behaviors. Non-syndromic KCOTs are uncommon and account for only 5% of the cases. The purpose of the present case report is to conduct clinical, radiographic and pathologic evaluations and treat a 37-year-old man with non-syndromic nevoid basal cell carcinoma. Syndromic and non-syndromic keratocysts present more invasive behaviors than the solitary type. The initial symptoms of syndromic keratocysts appear as multiple keratocysts of the mandible and maxilla that are diagnosed by a dentist; as a result, the diagnosis and treatment of the disease is very crucial.
Author Contributions
Academic Editor: Ioannis Chatzistefanou, 401 General Military Hospital of Athens
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Sohanian Shabnam, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Odontogenic keratocyst is a developmental odontogenic cyst that requires special considerations due to its histopathological features and invasive clinical behaviors. The WHO has recommended the term KCOT to be used as it better reflects the molecular genetic changes in the cyst, which resemble the changes in certain neoplasms 1.
Multiple odontogenic keratocysts are normally associated with concomitant cutaneous, skeletal, ocular and neurological anomalies as part of nevoid basal cell carcinoma syndrome or the Gorlin-Goltz syndrome, 2 although they may also be associated with the Simpson-Golabi-Behmel syndrome, the orofacial digital syndrome, the Noonan syndrome and the Ehler-Danlos syndrome 2, 3, 4, 5. Non-syndromic multiple odontogenic keratocysts are uncommon and only about 5% of the patients report this type 2.
KCOTs originate from the remnant of the dental lamina and normally affect a wide age range but affect men very little 1. The most common sites involved in odontogenic keratocysts include the posterior mandible body and the ramus areas 1. Its syndromic type usually occurs in the first decades of life and presents a higher risk of recurrence as well as more invasive behaviors compared to the non-invasive type. Odontogenic keratocysts may turn into invasive neoplasms such as ameloblastoma and squamous cell carcinoma. The syndromic and non-syndromic types of keratocysts are more invasive than the solitary types 6.
Given that multiple KCOTs are very rare and may be the first symptom of the syndromic condition and since the non-syndromic type is less common, the present study was conducted to perform clinical, radiographic and pathologic evaluations and treatment non-syndromic multiple KCOTs involving the mandible and maxilla in a 37-year-old man.
Case Report
The patient was a 37-year-old man who had undergone periodontal treatment eight years before due to gum disease. He presented to a dentist about two months ago complaining of the discharge of pus and a bad taste in his mouth, especially in his mandible. The clinical features showed no evidence of swelling (Figure 1 and Figure 2) and the dentist recommended a radiograph.
Figure 1.The patient’s clinical features
Figure 2.The patient’s intraoral view
The panoramic radiographs showed seven cysts in the mandible and maxilla. The patient was then referred to the surgical unit of the School of Dentistry. A CT scan was performed in order to better examine the patient and the images obtained revealed multiple extended cysts in the posterior and anterior mandible and maxilla with no swelling. The CT scan and panoramic radiographs showed multiple radiolucencies with well-demarcated borders, cortical margins and different sizes (Figure 3 and Figure 4). The interpretation of the radiographic images diagnosed the patient with radicular cysts and odontogenic keratocysts. The clinical examination of the patient revealed no systemic diseases or symptoms in the skin and the involved areas. The chest and skull radiographs also showed no symptoms.
Figure 3.The panoramic radiograph showing multiple cysts in the maxilla and mandible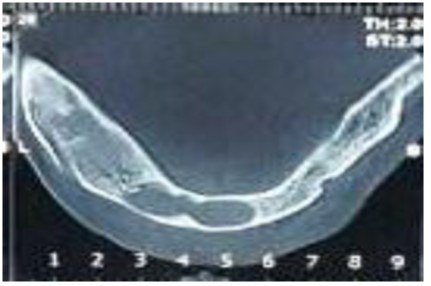
Figure 4.The axial cross-section of the CT scan showing radiolucencies with well-defined borders
According to the microscopic analysis of the incisional biopsy of the anterior mandibular lesion extending from the mesial left canine to the right first premolar, epithelial detachment from the connective tissues was observed in some areas of the cystic structure lined with para-keratinized stratified squamous epithelium. The connective tissue of the cyst wall was fibrocollagenous with diffuse infiltrates and the inflammatory cells were mainly chronic and comprised islands of odontogenic epithelium with a marginal band of cylindrical cells resembling ameloblasts. Blood vessels, nerves, muscles, extravascular hemorrhage and hemosiderin pigment were observed. The microscopic observations confirmed the diagnosis of inflammatory odontogenic keratocysts (Figure 5 and Figure 6). The patient underwent marsupialization in the symphysis and the lateral ramus for treatment and was then followed up with for the purpose of this study for 8 months.No recurrence was seen.
Figure 5.Hematxylin-eosin staining, Para-keratinized stratified squamous epithelium covering the inflammatory odontogenic keratocysts (×10)
Figure 6.Hematxylin-eosin staining, The odontogenic epithelium in the fibrocollagenous cyst wall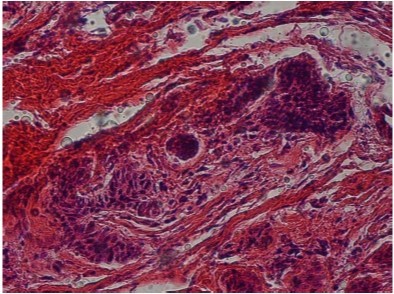
Discussion
Solitary keratocysts are more common than syndromic and non-syndromic multiple odontogenic keratocysts 4. Habibi et al. found no non-syndromic keratocysts of the 83 cases reported in the Iranian population and found only 8.3% of them to be syndromic 7. Brannon et al. reported that, of the 312 cases of keratocysts examined, 5.1% were syndromic and 5.8% were non-syndromic 8. Seifi et al. observed the second case of non-syndromic multiple keratocysts in the Iranian population in 2016 9. The case reported in this study was a 37-year-old man with non-syndromic multiple keratocysts in his mandible and maxilla, who complained of the discharge of pus and a bad taste in his mouth. The review of case reports of this condition showed that the non-syndromic type often affects the individual at early decades of life, mainly the second decade, with the mandible and maxilla being the most common sites of involvement, as in line with the present findings. Kurdekar 10 and Bartake 11found the maxilla to be the target area of non-syndromic keratocysts, which is inconsistent with this case report. Swelling, pain, drainage and discharge of pus and delays in tooth eruption have been reported as the causes of presenting with non-syndromic multiple keratocysts. The present case report is consistent with the results obtained by Bartake 11, Kurdekar 10 and Auluk et al. 3in terms of the symptoms of involvement, but inconsistent with the results obtained by Parikh 12.
This case report is on the third case of non-syndromic multiple keratocysts in the Iranian population as per the review of English articles on the subject in Iran. The non-syndromic type appears to be less common than the syndromic type in the Iranian population and ethnicity.
In cases such as this one, the question arises as to what the origin of non-syndromic multiple keratocysts is. Some researchers have proposed incomplete mutations in the PTCH tumor suppressor gene caused by the loss of an allele as responsible, since it inhibits the function of smoothened homolog (SMO). Other researchers attribute non-syndromic multiple keratocysts to the multifocal nature of keratocysts 3.
The present case report found no symptoms in the skin of the patient’s hands and legs and in his appearance in the clinical examination, and also no symptoms in his skull and chest radiographs. The radiographs in this case report showed seven well-circumscribed unilocular radiolucencies in the mandible and maxilla.
The case report presented by Bartake et al. showed non-syndromic multiple keratocysts and multiple radiolucencies with ill-defined borders in the maxilla 11. Rai et al. reported multiple radioloucencies with well-defined borders in both the mandible and maxilla 6.
The pathological features observed in this case report showed no satellite cysts in the connective tissue, although satellite cysts are believed to be more common in syndromic keratocysts than in non-syndromic cases. Epithelium is not the only factor involved in the recurrence and invasive behaviors of keratocysts and stroma and its agents seem to play a part too. Leonardi et al. reported a higher matrix metalloproteinases-13 expression in solitary keratocysts compared to in syndromic keratocysts and reported a negative expression in non-syndromic multiple keratocysts 13.
Cases of non-syndromic multiple keratocysts are reported mainly to highlight the importance of further examining therapeutic methods. Numerous therapeutic methods are used for the treatment of keratocysts, including simple curettage, enucleation, marsupialization and resection 14. Some researchers believe that marsupialization reduces inflammatory cytokeratins, especially IL1, in cases of multiple keratocysts 15. Resection and iliac crest grafts are used in cases where the lesion is too large 14. Marsupialization was used to treat the cases of non-syndromic multiple keratocysts reported and no recurrences were observed over a six-month period.
Conclusion
Despite the clinical, radiographic and pathologic differences among solitary, syndromic and non-syndromic keratocysts, the main finding of the present case report is that treatment and invasive behaviors differ in the syndromic and non-syndromic types.
References
- 1.Ahmed.Abdullah W.(2011) Surgical treatment of keratocystic odontogenic tumour: A review article.Saudi. , Dent J 23, 61-5.
- 2.Kargahi N, Kalantari M. (2013) Non-Syndromic Multiple Odontogenic Keratocyst: A Case Report. , J Dent Shiraz Univ Med Sci 14, 151-154.
- 3.Auluck A, Suhas S, Pai K M. (2006) Multiple Odontogenic Keratocysts:Report of a Case. , J Can Dent Assoc 72, 651-6.
- 4.Maheshwari V, Patel N, Jadhav R, Engineer P. (2015) Non-Syndromic Odontogenic Keratocyst: A Case Report. JDMS 1,64-67
- 5.Narsapur S A, Choudhari S, Warad N M, Manjunath S. (2015) Non-syndromic multiple odontogenic keratocysts associated with dental anomalies: A report of unusual case and its management. , J Indian Acad Oral Med Radiol 27, 268-72.
- 6.Rai S, Rana A S, Kalra P, Gupta D, Goel S. (2013) Multiple keratocystic odontogenic tumors in a non-syndromic minor patient: Report of an unusual case. , J Orofac Sci 5, 61-6.
- 7.Habibi A, Jafarzadeh H. (2010) basal cell carcinoma syndrome a 17 –year study of 19 cases in iranian population (1991-2008).Oral Pathol. , Med 39, 677-80.
- 8.Brannon R B. (1976) The odontogenic keratocyst. A clinicopathologic study of 312 cases. Part I. Clinical features. Oral Surg Oral Med Oral Pathol. 42, 54-72.
- 9.Seifi S,Moodi E,Hashemipour G,Fouroghi R,Nosrati K.( 1395)Two case reports of multiple keratocyst syndromic and non syndromic.JIDS 321:. 12-29.
- 10.Kurdekar RS,Prakash J,Rana AS,Kalra P. (2013)Non syndromic odontogenic keratocysts:A rare case report.National. , J Maxillofac Surg 4, 80-83.
- 11.Bartake A R, Shreekanth N G, Prabhu S.Gopalkrishnan K.(2011) Non-Syndromic Recurrent Multiple Odontogenic Keratocysts: A Case Report,J. , Dent(Tehran) 8, 96-100.
- 12.Parikh N R.Non-syndromic multiple odontogenic Keratocyst Report of case.(2010). , J Advanc Dent Res 2, 71-74.
- 13.Leonardi R.Mathews JB,Caltabiano R,Greco M,Lombardo C,Loreto C,et al(2010)MMP-13 expression in keratocyst odontogenic tumor associated with nevoid basal cell carcinoma and sporadic keratocysts.Oral. , Dis 16, 795-800.