
Hip Angle Behavior in Landing After Drop Jump in Children; and their Implicance in Prevention Programs
Abstract
Background
The Anterior Cruciate Ligament (ACL) injury is uncommon, but constitutes an important percentage of the lesions requiring more than 8 weeks of recovery in sports. Most ACL injuries do not require external contact and are associated with biomechanical risk factors that stress this ligament ACL: like an increase in knee valgus angle (KV) and hip flexion (HF) and a decreased in knee flexion (KF). The ACL requires muscle cooperation to resist the load; however, when there is fatigue, the protective capacity of the musculature would decrease. The objective of the study is to analyze the angular behavior before and after a physical load for HF in children of 14-15 years old.
Hypothesis
The physical load applied in a single training session is enough to change some biomechanical risk factors of ACL injury.
Study Design
Experimental study
Level of Evidence
2b
Methods
The sample consisted of 50 students from different soccer schools between 14-15 years old. We analyzed the hip angular behavior of hip flexion before and after a training session. The angles where obtained from inertioal sensor while the students performed a Drop Jump test from a 30 centimeters drawer.
Results
Statistically significant differences were found in the differences between pre physical load HF / post-load HF (p = 0.00053), right pre physical load HF / right post- load HF (p = 0.0086) and left post- load (p = 0.0248206).
Conclusions
It was concluded that the angular behavior of HF increases significantly in both post-training limbs, after performing a physical load.
Clinical Relevance
This study analyzed the importance of using prevention injury programs since early stages, and give importance to the eccentric role of hamstring, gluteus and core exercises.
Author Contributions
Academic Editor: Liye Zou, Department of Physical Education and Sports Science, The Chinese University of Hong Kong.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Jair Burboa G, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The Anterior Cruciate Ligament (ACL) lesion is classified as an uncommon lesion; however, it is characterized by the fact that a large percentage (47.8%) of the lesions require more than 8 weeks of recovery in sports, are due this kind of injury19.
In addition, 77.7% of cruciate ligament injuries were associated with sports, with 42.9% occurring during competitions and 34.8% in training12.
It is known that not all ACL injuries in sports require contact, in fact, a significant percentage occurs without external contact19. ACL non-contact injuries frequently occur during deceleration, leap landing or while turning to execute a lateral direction change2,17.
It is important to mention the existence of biomechanical risk factors which includes increased knee valgus (KV)1,28,7,15knee flexion (FR)13, increased hip flexion (HF)8 and increased ground reaction strength. This mechanism would increase the load on the ACL by inducing a more vigorous contraction of the quadriceps35.
Bowerman3related the effect of fatigue with the low muscle level response, suggesting that in a subject with fatigue the protective capacity of the musculature would be diminished. Wojtys29 examined adult, non-athletic and healthy subjects from which they observed that after inducing fatigue there was an increase in anterior tibial translation near 133N in both men and women. Skinner25 found similar results in the left leg, but not in the right, despite performing additional physical exercise. Rozzi23 observed that fatigue due to isokinetic exercises did not alter the anterior tibial translation therefore the influence is not very clear. It is also known that most soccer injuries occur during the last 15 minutes of the first half and the last 30 minutes of the second half of the competition, so fatigue could be an important factor9. There are clear contradictions between different authors as to whether or not the physical load plays a role in the production of injuries, so we are interest in answer the question, Does training loads plays a role in hip flexors angles risk factors for ACL injury? And also, is justified the use of core exercises in prevention programs at this ages?
The main objective has been to determine the angular behavior of the hip joint in the flexion, before and after applying a physical load, through a kinematic analysis by means of the inertial sensors of a Drop Jump (DJ) in children between 14-15 years old10.
The hypothesis of this study is whether the physical load in soccer increases the angle of hip flexion, after applying a physical load, in children who practice amateur soccer, between 14-15 years old.
Materials and Methods
Population
The populations for this study were 4 children's soccer schools located in Santiago, Chile. The inclusion criteria were to be born in the years 2004-2005 and practice 3-5 hours of soccer per week, while the exclusion criteria were to have a prior history of ACL rupture and joint or periarticular pathology in the 3 months prior to the test. The sample consisted of 50 individuals born in the years 2004-2005, who were chosen by convenience sampling. The sample data are summarized in Table 1.
Table 1. The sample data.| Variable | Mean ± Standard deviation |
| Age | 14.34 ± 0.51 years |
| Weight | 46.51 ± 8.71 Kg |
| Size | 152.04 ± 8.68 cm |
| Span (arms opens, from hand to hand) | 150.2 ± 8.65 cm |
| Foot size | 25.8 ± 1.38 cm |
Equipment Specifications and Software Features.
The tool for obtaining data was the MVN motion capture system consisting of 17 MTx sensors plus 2 Xbus Masters sensors. MTx is an inertial sensor and magnetic measurement unit comprising gyros, accelerometers and 3D magnetometers34, while the Xbus Masters has sensors such as the MTx that synchronize the data obtained and conduct the wireless connection with the computer. Sensor Modules (MTx) are placed on the feet, legs, pelvis, shoulders, sternum, head, arms, forearms, arms and hands21.
The initial position between the sensors and the body segments is unknown at the beginning, therefore, a calibration procedure has to be performed in which the alignment and body dimensions are determined22.There is no limitation by occlusion with the surrounding objects or by other people who are interacting with the study subject. The subjects are not obliged to a specific volumetric measurement, needing only the height, span and length of the subject's foot. It also has the advantage that their movements can be measured in an environment that is familiar to them when performing their daily tasks22.
Data Collection
Procedures
An Experimental, Transversal and Non-random study was carried out. Eight days of measurements were performed maintaining a specific order. First, the players were summoned to their regular training location with their usual soccer shoes. Then, a previous measurement was made in order of arrival in which the first child measured in the previous phase would be measured in the later phase so as to achieve the same amount of training in minutes. The placement of Xsens MVN sensors was done next by means of a protocol to be observed at a later point in the text 2.3.3). Finally the subjects were instructed to perform a drop jump (DJ) test that consisted in the drop of a drawer of 0.3 m height with both feet at the same time on a hoop located 0.5 m distance. Each subject had to perform at least 3 DJ jumps. Once the subject has completed the three jumps, the Xsens MVN sensors are removed in order to be used by the next subject.
Drop Jump
It is a test that allows evaluating the reactive force of the lower limbs. The subject must perform a vertical jump action after a fall of a drawer, in this study, the drawer has 30 cms. The fall must be advancing one foot while leaving the rest to the gravitating effect so as not to alter the height of the fall4. The action of the arms will not be taken into account in this study because the phase to be evaluated will be that of shock absorption, a phase in which the action of the arms is negligible5
Position of the Inertial Sensors
The sensors were placed as indicated by the manufacturer. Two Master Xbus sensors were placed the posterior superior iliac spine and six MTx sensors located at the functional rotation point of each joint under study, using as reference points the greater trochanter of the femur, tuberosity of the tibia and the ankle-talus joint center, so that by connecting all the joint centers a skeleton is formed in the software used by Wu31, 32,33.
Training Protocol
Pre Competition
Development of low intensity exercises which combine a slow jog with joint mobility for upper and lower extremities. Afterwards, the intensity of the jog is increased and when the auditory signal (whistle) is given the subjects must perform actions such as jumps, dribbling and changes of direction. Then, there are 3 sets with 4 repetitions of 35 meter sprints. The final exercise consists of the subjects forming lines and when a tactile, auditory or visual signal is given, they must perform speed sprints; 3 series of 5 repetitions at a distance of 15 meters. This stage lasts approximately 25 minutes.
Technical Physical Work
An important physical component is combined with a technical one, which consists of 3 different tasks with duration of 12 minutes each. The first exercise is an aerobic component of controlling the soccer ball in addition to controlled passes in a circuit of 20 meters one way and 20 meters return. The second exercise consists of a coordination work along with technical sequences and vertical jumps that end with 30 meter speed sprint races (3 series). The third exercise consists of reduced soccer (4 vs 4) which has duration of 15 minutes.
Reality of Game
Soccer is played in dimensions that match the age (50x30 meters). This stage lasts 20 minutes per time with a break of 5 minutes. After the last measurement, the final exercise consists of the children performing a 15-minute regeneration jog followed by passive-active type stretching for all muscle groups most used in soccer practice such as the hip and knee flexors and extensors, abductors and sural triceps in 3 sets of 20 seconds per muscle group.
Obtaining Angular Peaks
The angular peak corresponds to the maximum angle reached by a joint at any given moment during any movement. The angular peaks in the hip joint were obtained in the hip flexion (HF) for the left and right legs. Each test subject performed 3 jumps of DJ pre physical load and post physical load, although for purposes of this study, only 1 angular peak was taken which was the highest value reached in any of the 3 executions, leaving 1 angular peak for the following variables. HF pre-physical load 26.27 ± 10.39°, HF post physical load 31.04 ± 12.91°.
For this study, the variables were divided into right and left extremities, thus working with 4 more variables whose values are right HF pre physical load 24.80 ± 10.28 degrees, left HF left pre physical load 27.24 ± 10.19º; right HF post physical load 29.82 ± 12.81°, left HF post physical load 32.26 ± 12.76°, Summary in Table 2.
Table 2. Summary of angular peaks.| Variable. | Mean/Standard deviation. |
| HF pre physical load. | 26.27± 10.39º |
| HF post physical load. | 31.04± 12.91º |
| HF right pre physical load | 24.80± 10.28 |
| HF left pre physical load | 27.24± 10.19º |
| HF right post physical load. FR right pre physical load | 29.82±12.81º63.50± 11.58º |
| HF left post physical load. FR left pre physical load. | 32.26± 12.76º65.67±10.27º |
Statistical Analysis
The value to be analyzed will be the difference between the angular peak post physical load and the angular peak pre physical load. In order to determine the normality of the sample, the Shapiro Wilk test will be applied. The variables that present normal distribution will be analyzed with the t student test for paired samples, whereas those that do not show a normal distribution will be analyzed with the Wilcoxon test. A statistically significant difference was observed for a p <0.05 value. The statistical analysis was performed using the Statgraphics Centurion XVI.I., data analysis program.
Instrument Validation
The use of inertial sensors is supported by the Cuesta-Vargas6 systematic review, in which the inertial sensors are compared with bio-instruments electrogoniometry, optoelectronic systems, electromagnetic systems, etc.) concluding that inertial sensors can provide an accurate and reliable method for studying human movement24. They are able to measure different areas of the body and overcome the problem of scope or the metallic disturbance associated with other methods; provide a tool that has the potential to encompass many applications in different environments; provide the capacity for data collection outside the laboratory so that studies that require evaluation of motor gestures will be able to be performed in the subject's own environment delivering more reliable and accurate data.
Ethical Considerations
The study participants had to sign an informed consent as well as their tutors which were reviewed and approved by the ethics committee of the Metropolitan University of Education Sciences on September 10, 2018.
Results
In the comparison of HF pre physical load with HF post physical load, it was observed that the angular average for the pre-load phase was 26.27º, while the angular average for the post-load phase was 31.04º, with the 4.77 ° increase being statistically significant (Figure 1). When analyzing the right angular HF for the pre physical load phase was 24.80 degrees while the angular average for the post-load phase was 29.82 degrees. This increase of 5.02 degrees is statistically significant (Figure 2). In left HF, the angular average for the pre physical load phase was 27.74 degrees while the angular average for the post physical loading phase was 32.26 degrees with this 4.52° increase being statistically significant (Figure 3).
Figure 1.Comparison of HF pre physical load with HF post physical load.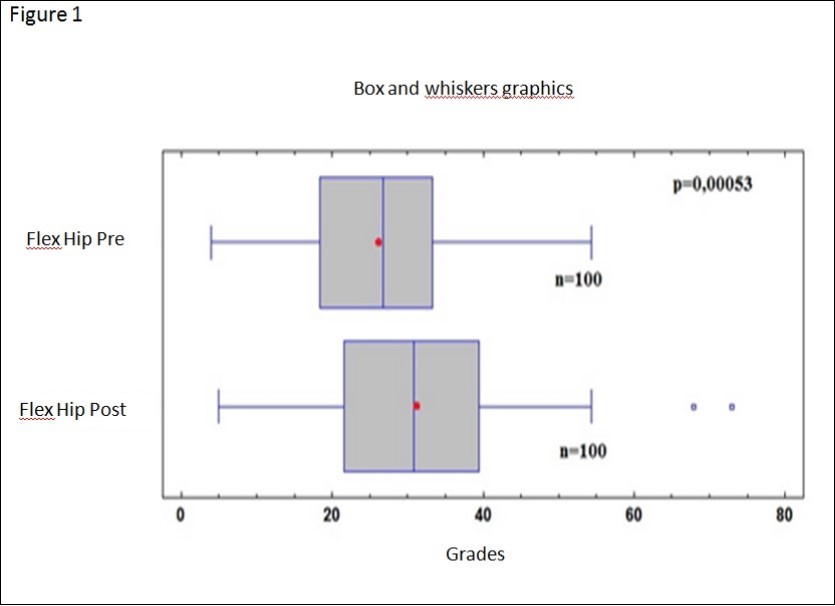
Figure 2.Comparison or right HF preload physical with right HF post physical load.
Figure 3.Comparison HG left physical preload with left HF after physical load.
Discussion
In the present study, we evaluated male subjects from 14 to 15 years of age, belonging to 4 children's soccer schools. The participants are in a formative age of the trained sport, for which it has a recreational objective as well as the future objective of reaching their maximum performance in adulthood, for which they are improving the physical performance, acquiring technique and perfecting motor gestures.
The tool used to evaluate the angular behavior was the Xsens MVN inertial sensor, which as demonstrated in previous research has a high reliability in the measurement of the studied biomechanical variable.
The participants were subjected to standardized training that is similar to the one performed each week, which seeks to control the load exerted on them. Furthermore, the gesture with which it was evaluated, the Drop Jump (DJ), requires the landing, that is also an activity that is frequently requested in soccer, reason why they were not submitted to tasks other than the commonly done. Finally, all the evaluations were made in a familiar atmosphere, the training place they use to practice and with their usual equipment.
As for the results obtained in hip flexion, it was observed that in the total of the sample there was an increase of 4.77°, with 5° in the left leg and 4.6° in the right leg. These were statistically significant increases, which is why the increase of the biomechanical variable is associated with the physical load exerted20. It is important to note that the results are within the range of HF established in the study of Boden2, in which the gesture performed in soccer players at the moment of having an ACL rupture was studied by videophotogrammetry. In this study2 the angle of the hip at the time of injury was more flexed in the study group (injury) than in the control group (non-injured), which provides a guideline that an increase in hip flexion after a landing may increase the incidence of ACL injury. The interval in which the subjects had ACL rupture was set between 17-31 degrees of hip flexion. In the case of our study, the average values before training for left and right leg were 24.8 and 27.7 and after training were 29.82 and 32.36 respectively, which will be within the range where the injury of ACL could occur. There is a statistically significant increase for the pre-training and post-training difference in these values, so the poorly performed gesture, together with the increased hip flexion angle, could be associated with a potential risk of ACL injury14.
Regarding the reference values that exist for the angular behavior, these are derived from measurements made in adult subjects, and therefore they are not applicable for the study population. In spite of this it is of utmost importance to establish the existing relationship for the correction of motor gestures that are being acquired.
Regarding hip analysis, although it is a variable that could be related to a potential risk of ACL injury, is the least studied in the literature. However, increased hip flexion may be due to decreased eccentric strength of gluteus maximums and hamstring muscles, since according to the study27, in the fall of a jump with a horizontal component, these would be the muscles most requested for the maintenance of the hip position. Considering that the semitendinosus and semimembranosus hamstring muscles are ACL agonists and hip extensors, we could associate the fatigue of these muscles with the increase of hip flexion angle and a potential risk of cruciate ligament injury due to weakness in the load performed during training.
Another important factor at hip level is the position since according to the results obtained in the study18 men who are at the age of our study subjects would have a tendency for pelvic anteversion, a position which would be mechanically unfavorable for the action of the muscles of the posterior chain. This isn`t been analyzed in our population.
There a lack of studies in children aged 10 to 14 years in the literature concerning prevention of this type of injury. Soccer is among the sports most commonly played by patients from 5 to 17 years of age who tear their ACLs26. Greater laxity (changes in passive elements), combined with the physiological changes that occur during puberty (for example neuromuscular control), could affect the type, severity and incidence of lesions in the adolescent population. In addition to this, children may be more susceptible to an injury due to excess exposure to athletic training than adults due to the growth of cartilage tissue and the growth process itself. The data supports the idea that the puberty period of rapid growth and development in children can be a significant factor of injury patterns in sport and therefore injury prevention efforts should be targeted at youth before the onset of puberty. A recent meta-analysis of ACL injury prevention studies concluded that greater success in reducing knee injury in athletes was achieved through preventive neuromuscular training that began before the onset of neuromuscular deficits and the peak incidence of knee injuries in adolescents16. It would be optimum if it is performed during the first ages of sport participation, since the neuromuscular training performed during or before pre-adolescence, increases the neuromuscular function related to the improvement of biomechanical movements that can lead to a reduction of knee ACL injuries26. For this reason, the FIFA Medical Evaluation and Research Center (F-MARC), along with a group of international specialists, created the FIFA 11+ program to be used in order to prevent injuries in the lower extremities and improve performance in people who play soccer.
The training done in a standard way to the students of the participating soccer schools is similar to the one commonly executed on training days, either in terms of duration and type of work to be performed. Furthermore, the place where the evaluation was carried out is where they routinely carry out their training sessions, which will positively influence various types of variables such as moderators (footwear and training surface) since the individuals used the same footwear they occupied in all their training sessions. In addition to the latter, the surface used for the test is the same as the one used to perform all their training sessions. The unknown variables (psychological status, stress and motivation) are also positively influenced by the fact that they were in a well known environment during their normal practice, in addition to the motivation received by their teachers and parent. Psychological and stress factors were favored in the control of these variables.
Regarding the use of the Xsens MVN sensor equipment, the children were consulted about any discomfort they might have presented with their use, so that this would not interfere with the jump process. Furthermore, the weight of the sensors (less than 2 kg.) that was distributed throughout the lower extremity was negligible for the individuals. No discomfort was experienced when using the Xsens MVN sensors at the time of jumping performance.
In reference to the bias of our study, we found some variables that were not controlled, such as the time it takes to train each child in his respective school, so that the level of experience or expertise in the movements he/she can perform are not fully controlled thus, having individuals with better technical gestures than others and therefore better control of the motor gesture. The type of footwear that the children used were not controlled either, so it was not the same for all thus creating variations when the DJ was performed. Other variables of interest are the state of fatigue, which could be measured with electromyography or fatigue scale (Borg), which is suggested to be controlled in future investigations, as well as a postural evaluation seeking pelvic antevertion.
Conclusion
The resulting physical load after training improved the hip flexor angle in boys aged 14 to 15 years playing amateur soccer.
Our results reflect the effects of the fatigue of a training session thus alter the biomechanical risk variables of a ACL injury, increasing the hip flexor angles, this could reflect a lack of eccentric strength in the gluteus maximums and hamstrings, as well as a lack of trunk control in men aged 14 to 15 years practicing amateur soccer.
References
- 1.Arms S W, Pope M H, Johnson R J, Fischer R A, Arvidsson I et al. (1984) The biomechanics of anterior cruciate ligament rehabilitation and reconstruction. , Am J Sports Med.12: 8-18.
- 2.Boden B P, Torg J S, Knowles S B, Hewett T. (2009) Video analysis of anterior cruciate ligament injury. , The American Journal of Sports Medicine 37, 252-259.
- 3.Bowerman S J, Smith D R, Carlson M, King G. (2006) A comparison of factors influencing ACL injury in male and female athletes and non-athletes. , Phys. Ther. Sport 7, 144-152.
- 4.Bosco C, Luhtanen P, Paavo V. (1983) A simple method for measurement of mechanical power in jumping.European. , Journal of Applied Physiology and Occupational Physiology 50, 273-282.
- 5.Bosco C, Komi P V, Ito A. (1981) Prestretch potentiation of human skeletal muscle during ballistic movement.ActaPhysiolScand.111:. 135-140.
- 6.Cuesta-Vargas A I, Galán-Mercant A, Williams M J. (2010) Systematic Review. The use of inertial sensors system for human motion analysis. Physical Therapy Reviews. 15, 462-473.
- 7.Fleming B C, Beynnon B D, Renstrom P A, Engstrom B, Peura G D. (2001) The effect of weightbearing and external loading on anterior cruciate ligament strain. , J Biomech 34, 163-70.
- 8.Hashemi J, Breighner R. (2011) Chandrashekar N - Hip extension, knee flexion paradox: a new mechanism for non-contact ACL injury. , J. Biomech 44, 577-585.
- 9.Hawkins R D, Fuller C W. (1999) A prospective epidemiological study of injuries in four English professional football clubs. , British journal of sports medicine 33, 196-203.
- 10.Herrington L, Munro A. (2010) Drop jump landing knee valgus angle; normative data in a physically active population. Physical Therapy in. , Sport 11, 56-59.
- 11.Jefferson R, Collins J, Whittle M, Radin E, O'Conner J. (1990) The role of the quadriceps in controlling impulsive forces around heel strike. , Proc IMechE Part H J Eng Medi 204, 21-28.
- 12.Kobayashi H, Kanamura T, Koshida S, Miyashita K, Okado T. (2010) Mechanisms of the anterior cruciate ligament injury in sports activities: A twenty-year clinical research of 1,700 athletes. , Journal of Sports Science and Medicine 9, 669-675.
- 13.Krosshaug T, Nakamae A, Boden B P, Engebretsen L, Smith G et al. (2007) . , Mechanisms of Anterior Cruciate ligament Injury in Basketball. The American Journal of Sports Medicine 35, 359-367.
- 14.Lin C F, Liu H, Gros M T, Weinhold P, Garrett W E et al. (2012) Biomechanical risk factors of non-contact ACL injuries: A stochastic biomechanical modeling study. , J. Sport Heal. Sci 1, 36-42.
- 15.McLean S G, Huang X, AJ Van den Bogert. (2008) Investigating isolated neuromuscular control contributions to non-contact anterior cruciate ligament injury risk via computer simulation methods. , Clin. Biomech. (Bristol, Avon) 23, 926-36.
- 16.Myer G D, Sugimoto D, Thomas S, Hewett T E. (2013) The influence of age on the effectiveness of neuromuscular training to reduce anterior cruciate ligament injury in female athletes: a meta-analysis. , Am J Sports Med 41, 203-215.
- 17.Myklebust G, Engebretsen L, Bahr R. (2004) Injury Mechanisms for Anterior Cruciate Ligament Injuries in Team Handball. A Systematic Video AnalysisOdd-Egil.
- 18.Nguyen A, ShultzS SchmitzR. (2015) Landing biomechanics in participants with different static lower extremity alignment profiles.J.AthlTrain.50:. 498-507.
- 19.Paús V, Del Compare P, Torrengo F. (2003) Incidencia de lesiones en jugadores de fútbol profesional. Revista de la Asociacion Argentina de Traumatologia del Deporte. 10, 10-17.
- 20.Podraza J T, White S C. (2010) Effect of knee flexion angle on ground reaction forces, knee moments and muscle co-contraction during an impact-like deceleration landing: implications for the non-contact mechanism of ACL injury. , Knee 17, 291-295.
- 21.Roetenberg D, Luinge H, Slycke P. (2009) Xsens MVN: full 6DOF human motion tracking using miniature inertial sensors. Xsens Motion Technologies BV. Tech. Rep
- 22.Rotenberg D, Chiew M, Ranieri S, Tam F, S Chopra R Graham. (2013) Real-Time Correction by Optical Tracking with Integrated Geometric Distortion Correction for Reducing Motion Artifacts in Functional MRI. , Magnetic Resonance in Medicine 69, 734-748.
- 23.RozziS LephartS, Fu F. (1999) Effects of Muscular Fatigue on Knee Joint Laxity and Neuromuscular Characteristics of Male and Female Athletes. , J Athl Train 34, 106-114.
- 24.Saber-Sheikh K, Bryant E C, Glazzard C, Hamel A, RYW Lee. (2010) Feasibility of using inertial sensors to assess human movement. , Manual Therapy 15, 122-125.
- 25.Wyatt MP SkinnerHB, Stone M L, Hodgdon J A, Barrack L. (1986) Exercise-related knee joint laxity.Am. , J Sports Med 14, 30-34.
- 26.Stracciolini A, Stein C J, Zurakowski D, Meehan W P, Myer GDMicheli LJ. (2015) Anterior Cruciate Ligament Injuries in Pediatric Athletes Presenting to Sports Medicine Clinic: A Comparison of Males and Females Through Growth and Development. , Sport Healt 7, 130-136.
- 27.Struminger A H, Lewek M D, Goto S, Hibberd E, Blackburn J T.(2013).Comparison of gluteal and hamstring activation during five commonly used plyometric exercises.Clin Biomech. , (Bristol, Avon) 28, 783-789.
- 28.Withrow T J, Huston L J, Wojtys E M, Ashton-Miller J A.(2006).The effect of an impulsive knee valgus moment on in vitro relative ACL strain during a simulated jump landing.lin Biomech. , (Bristol, Avon) 21, 977-983.
- 29.Wojtys E M, Wylie B B, Huston L J. (1996) The effects of muscle fatigue on neuromuscular function and anterior tibial translation in healthy knees.Am. , J Sports Med 24, 615-621.
- 30.Whittle M. (1999) Generation and attenuation of transient impulsive forces beneath the foot: a review. , Gait Posture 10, 264-75.
- 31.Cavanagh P WuG. (1995) ISB recommendations for standardization in the reporting of kinematic data.Journal of Biomechanics,28:. 1257-1261.
- 32.Wu G, Siegler S, Allard P, Kirtley C, Leardini A et al. (2002) ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion - Part I: ankle, hip, and spine. , Journal of Biomechanics 35, 543-548.
- 33.Wu G, Helm F Van der, Veeger H, Akhsous M, P Van Roy et al. (2005) ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion- Part II: shoulder, elbow, wrist and hand. , Journal of Biomechanics 38, 981-992.