
An Assessment of The Knowledge, Risk Perception and Attitudes of Healthcare Workers in A Tertiary Health Facility in Southwest Nigeria to The Covid 19 Pandemic
Abstract
Aim
Covid 19 is a pandemic that has ravaged the world resulting in thousands of deaths. This study aims to assess the knowledge, risk perception, and attitude of health care workers (HCWs) to the pandemic.
Methodology
This was a hospital based descriptive cross sectional study conducted among health care workers who were staff of the hospital. Data collected includes socio demographic characteristics, data on knowledge, risk perception and attitude.
Results
A total of 288 HCWs participated in the study. Participants had good knowledge at 95.6%, major source of knowledge includes internet/social media 68.8%, radio 34.6% and television 28.3%. About 92.6% of the respondents also had positive attitude while 89.75 of the respondents had a positive risk perception.
Conclusion
Overall, there was a high level of knowledge, high positive attitude and a high risk perception in the study. Consequently, to ensure that this high level is maintained, there is need for continuous health education and promotion.
Author Contributions
Academic Editor: Ian James Martin, Edith Cowan University, USA
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 Adeniyi MA, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARSCoV-2), is the pathogen that causes coronavirus disease2019 (COVID-19), and is one of the most contagious viruses in human history1,2It is a highly communicable viral respiratory infectious disease with potential life-threatening complications.3,4,5It is a single-stranded RNA virus that belongs to the family of coronaviridae and it is commonly transmitted through contact with infected respiratory droplets.3,6,7 The incubation period of COVID-19 is 1 – 14 days while its common symptoms include fever, cough, dyspnoea and headache.1,3,4In addition, severe COVID-19 disease can lead to serious complications such as encephalitis, acute myocardial infection, renal failure, and multi-organ failure.1,2,4,7
There is no specific treatment for this disease, so health care providers treat the clinical symptoms (e.g. fever, difficulty inbreathing) which the patients present with. Supportive care (e.g. fluid management, oxygen therapy, etc.) can be highly effective for patients with symptoms.8
The first reported case of Covid-19 in Nigeria was in Lagos and this was reported by the Federal Ministry of Health on the 27th of February, 2020.10 As at 8th June, 2020 over 800 healthcare workers in Nigeria has been infected with the disease.11 As at 16th of September, 2020 there are 56604 confirmed cases with 1091 deaths.9Since the outbreak the Nigerian government, like other global community adopted measures to contain the spread of the disease. Some of these measures include social distancing, ban on public gathering including religious gatherings, continuous personal hygiene such as hand washing and use of hand sanitizers; use of face masks, limiting number of passengers in public vehicles, locking down public places etc.18These measures have not been effective due partly to lack of government enforcement, poor knowledge and attitude of the citizen.
Statement of Problem
Globally, around 14% of COVID-19 cases reported to WHO are among health workers, and in some countries it’s as much as 35%. The WHO estimates that over 41,000 health workers in Africa have been infected with COVID-19 as at 17/09/2020.19
Benefit
It is hoped that this study will help to improve the knowledge of HCWs, make HCWs more aware and have a better understanding of the risks inherent in the Covid 19 pandemic and thereby improve their attitude and with an improved attitude reduce the risk of infection with Covid 19.
It is also hoped that this research will enable policy maker make informed and evidence based policies to better the lot of HCWs in the hospitals and the communities at large.
Furthermore, a better knowledge, a better understanding of the risks and a good attitude will make adherence to the preventive protocols put in place by the government and respective hospital managements easy to adhere to and follow.
Objectives
This study aims to assess the knowledge risk perception and attitude of healthcare workers in a tertiary health facility to the Covid 19 pandemic
Methodology
This is a descriptive cross sectional study carried out in a tertiary health centre located in Ido – Osi Local Government Area of Ekiti State. The study targets HCWs who are staff of the facility.
Ekiti State is located in the South-western part of Nigeria. Ido Ekiti town is the capital of Ido – Osi LGA which is one of the 16 LGAs in Ekiti State. It is also a semi – urban LGA.12Ido-Osi LGA lies within latitude 7046.715’N and 7055.822’N and longitude 508.410’E and 5014.416’E.13 The study was carried out in the Federal Teaching Hospital Ido-Ekiti which is one of the three tertiary health facilities located within the state. The other two tertiary health centres are located in the state capital Ado – Ekiti.12
Ido – Osi local Government is basically agarian with people cultivating root crops and grains such as yams, cassava, maize, rice etc. There are a few cottage industries in the local Government devoted primarily to processing of Agricultural produce. Other industrial undertaking is in the area of printing, bakeries, weaving, carpentry etc.12
Sample Size Determination
n = Z2 x P (1 - P)/ E2
Where Z standard normal deviate at 95% = 1.96
P proportion of HCW with good knowledge in a similar Study = 78.615
E Level of error = 5%

For non-response rate compensation
ns = n/0.9
ns = 259/0.9
= 288
Therefore, 288 HCWs participated in the study
Sampling Technique
All consenting HCWs in the tertiary health facility were recruited for the study until the sample size was met. Self-Administered Questionnaires were administered on them within the hospital premises.
Sampling Instrument / Tool
Data was collected using pre tested semi-structured self-administered questionnaires which was administered by the researchers and their trained assistants.
Pre testing of the questionnaire was done at the Ekiti State University Teaching Hospital (EKSUTH) located at Ado Ekiti. Which is also a tertiary health care facility.
Study Variables
Independent Variable
Socio demographic characteristics
Dependent Variables
knowledge, risk perception and attitude.
Data Analysis
Filled questionnaires were sorted and data was analysed using Statistical Package for Social Sciences (SPSS) version 22. Data were then presented in the form of frequency tables, cross tabulation using chi-square. Bivariate analysis was done as applicable. Level of significance was set with P-value less than 0.05.
Inclusion And Exclusion Criteria
Inclusion Criteria
All consenting health care workers who are staff of the hospital.
Exclusion Criteria
Patients, visitors and all non-staff were excluded.
Ethical Consideration: Ethical approval for this research was gotten from the Human Research and Ethics Committee of the Federal Teaching Hospital, Ido-Ekiti. Verbal Informed consent was gotten from all the respondents and only those who consented were recruited for the study.
The study was carried out between August 2020 and April 2021.
Results
Table 1 shows the Socio demographic characteristics of the study participants. The total number of HCWs surveyed was 272. Among them, 118 (43.4%) were between the age of 30-39 years, the mean ± SD is 37.78 ± 8.17 with a range of 20 – 58.
Most of the respondents surveyed were female 164 (60.3%) while 118 (69.1%) had tertiary education qualification. Similarly, most of the HCW surveyed were nurses 88 (32.4%) Figure 1
Table 2 and Figure 2 most of the respondents surveyed 260(95.6%) had good knowledge of Covid 19
Table 3 and Figure 3 showed that most of the respondents surveyed had positive attitude 252 (92.6%) while Table 4 and Figure 4 showed that risk perception among most of the respondents were positive 244 (89.7%).
Table 4 and Figure 4 shows the risk perception of the HCWs to Covid 19. A greater percentage of the HCWs 244(89.3%) had a positive risk perception while only 28(10.3%) had a negative perception.
Table 5 showed the association between socio demographic characteristics and attitude with marital status found to be significantly associated with attitude at a p-value of 0.020 with divorce and single respondents having the highest value of 100% and 97.7% respectively. Similarly, the cadre of the respondents was also found to be significantly associated with attitude at a p value of 0.003 with doctors and laboratory scientist having a value of 100% each.
Table 6 showed the association between socio demographic characteristics and risk perception. This study found sex to be of significant association with risk perception at a p value of 0.013 with males having a higher positive risk perception 103 (95.4%) than females 141 (86%). Also, years of practice was found to be significantly associated with risk perception at a p value of 0.009 with those who have been in practice for more than 10 years having the highest value of positive risk perception at 122 (91.7%).
Table 7 shows the association between socio demographic characteristics and knowledge. This study found that 17(81%) , 180(95.7%) and 63(100%) of the respondents with secondary, tertiary and post tertiary education respectively had good knowledge of Covid 19 at a significant p value of 0.005. Similarly, there was also a significant association between years of practice and knowledge at a p value of 0.038 where 52 (91.4%), 76(93%) and 131(98.5%) of the respondents with <5 years, 5-10 years and >10 years, years of experience post graduation had good knowledge showing a progressive increase in the percentage with increasing years of experience.
Table 8 shows the association between knowledge, attitude and risk perception. This study found that there was a significant association between knowledge and risk perception at a p value of 0.025.
Figure 1.Knowledge of COVID 19 among the healthcare workers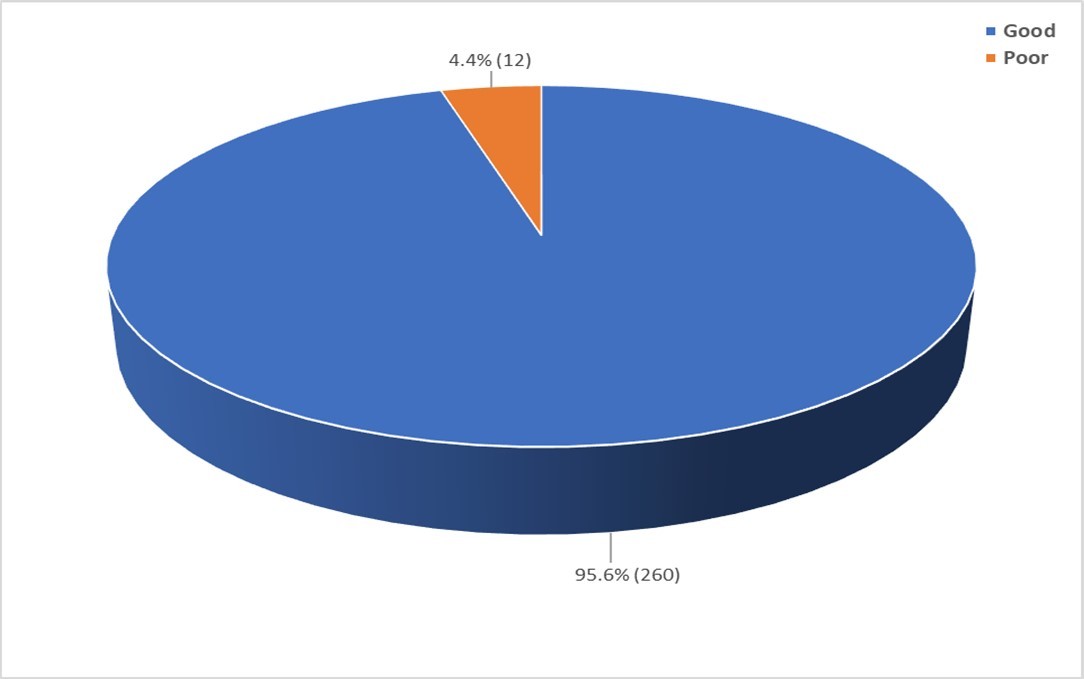
Figure 2.Source of knowledge about COVID 19
Figure 3.Attitude of health care workers to COVID 19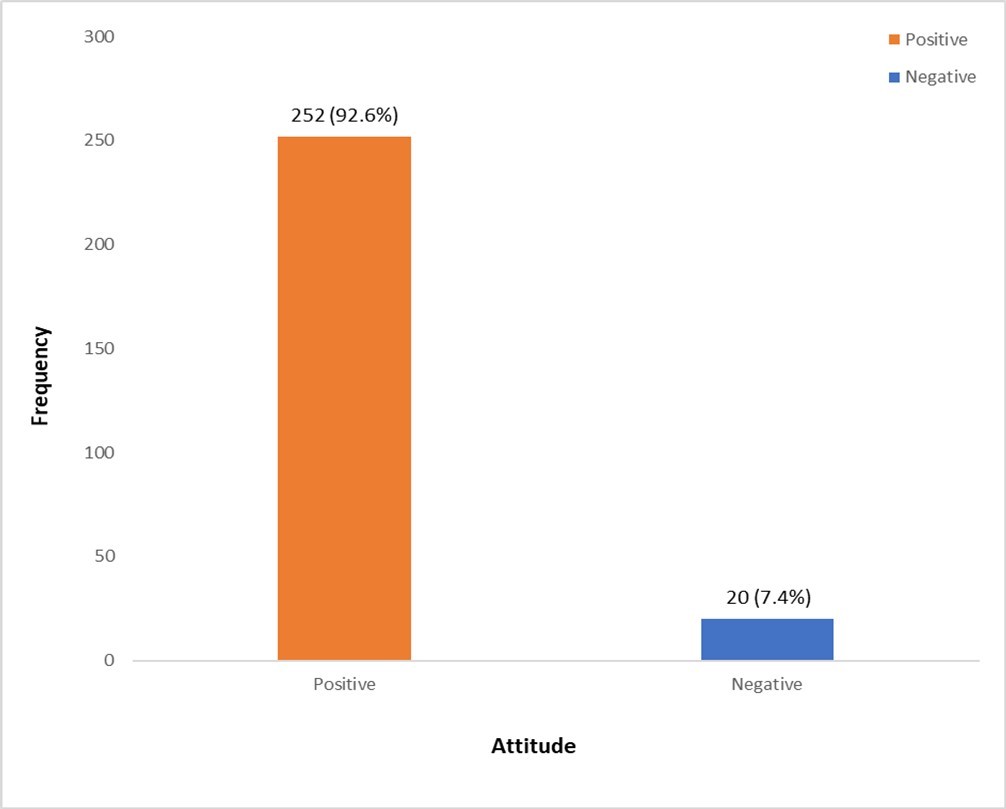
Figure 4.Overall risk perception of health workers to COVID 19
| Variable | Frequency | Percent |
|---|---|---|
| Age (years) | ||
| 20 – 29 | 41 | 15.1 |
| 30 – 39 | 118 | 43.4 |
| 40 – 49 | 81 | 29.8 |
| 50 – 59 | 32 | 11.8 |
| Mean ± SD | 37.78 ± 8.17 | |
| Range | 20 – 58 | |
| Sex | ||
| Male | 108 | 39.7 |
| Female | 164 | 60.3 |
| Educational qualification | ||
| Secondary | 21 | 7.7 |
| Tertiary | 188 | 69.1 |
| Post Tertiary | 63 | 23.2 |
| Marital status | ||
| Single | 44 | 16.2 |
| Married | 222 | 81.6 |
| Divorced | 3 | 1.1 |
| Widow/ widower | 3 | 1.1 |
| Religion | ||
| Christianity | 262 | 96.3 |
| Islam | 7 | 2.6 |
| Traditional | 3 | 1.1 |
| Tribe | ||
| Yoruba | 248 | 91.2 |
| Ibo | 10 | 3.7 |
| Hausa | 5 | 1.8 |
| Others | 9 | 3.3 |
| Cadre | ||
| Doctors | 73 | 26.8 |
| Nurses | 88 | 32.4 |
| Pharm | 6 | 2.2 |
| Lab | 14 | 5.1 |
| CHEW | 36 | 13.2 |
| Health attendants | 41 | 15.1 |
| Others | 14 | 5.1 |
| Years of practice | ||
| < 5 Years | 58 | 21.3 |
| 5 - 10 Years | 81 | 29.8 |
| > 10 Years | 133 | 48.9 |
| Knowledge of COVID 19 | n (%) | n (%) |
|---|---|---|
| Have you ever heard of the COVID 19 is 1 to 14 | 272(100) | 0(0.0) |
| Do you know that the COVID 19 pandemic is caused by SARS cov 2 | 186(68.4) | 86(31.6) |
| Do you know that the COVID 19 pandemic was first reported in Wuhan China | 239(87.9) | 33(12.1) |
| The incubation period of COVID 19 is 1 to 14 days | 253(93..0) | 19(7.0) |
| The virus is spread mainly from person to person | 254(93.4) | 18(6.6) |
| The virus is also airborne | 234(86.0) | 38(14.0) |
| The following are some of the symptoms of COVID 19- cough, fever and difficulty in breathing | 260(95.6) | 12(4.4) |
| There is no known drug for COVID 19 | 223(82.0) | 49(18.0) |
| Use of hand sanitizer and face mask can prevent the infection | 262(96.3) | 10(3.7) |
| Regular hand washing and physical social distancing can help prevent the spread of the disease | 266(97.8) | 6(2.2) |
| Presence of underlying illness such as hypertension and diabetes can make the infection more severe | 248(91.2) | 24(8.8) |
| SA | A | N | SD | D | |
| Attitude | n (%) | n (%) | n (%) | n (%) | n (%) |
|---|---|---|---|---|---|
| Do you agree that COVID 19 will eventually be successfully controlled | 123(45.2) | 134(49.3) | 10(3.7) | 2(0.7) | 3(1.1) |
| In your opinion will good personal hygiene reduce the risk of COVID 19 infection | 106(39.0) | 144(52.9) | 12(4.4) | 7(2.6) | 3(1.1) |
| Do you agree that guidelines from the hospital COVID 19 taskforce will help in controlling the disease in the hospital | 113(41.5) | 123(45.2) | 22(8.1) | 4(1.5) | 10(3.7) |
| Will you work or live with people who have been infected with COVID 19 | 29(10.7) | 69(25.4) | 55(20.2) | 51(18.8) | 68(25.0) |
| People infected with COVID 19 are careless with their health | 22(8.1) | 36(13.2) | 29(10.7) | 87(32.0) | 98(36.0) |
| COVID 19 infected individuals should be isolated even after treatment | 20(7.4) | 41(15.1) | 32(11.8) | 77(28.3) | 102(37.5) |
| COVID 19 can be transmitted through sexual intercourse | 34(12.5) | 56(20.6) | 30(11.0) | 67(24.6) | 85(31.3) |
| People infected with COVID 19 should not be allowed to come to work | 113(41.5) | 99(36.4) | 29(10.7) | 12(4.4) | 19(7.0) |
| Tuberculosis/Leprosy is better than COVID 19 | 31(11.4) | 67(24.6) | 54(19.9) | 56(20.6) | 64(23.5) |
| COVID 19 is a punishment from God | 28(10.3) | 26(9.6) | 35(12.9) | 120(44.1) | 63(23.2) |
| Risk perceptions | n (%) | n (%) |
|---|---|---|
| COVID 19 is a severe debilitating infection | 237(87.1) | 35(12.9) |
| COVID 19 is highly infectious | 257(94.5) | 15(5.5) |
| COVID 19 can cause respiratory failure | 251(92.3) | 21(7.7) |
| COVID 19 can cause severe diarrhea | 161(59.2) | 111(40.8) |
| COVID 19 can cause severe dehydration | 199(73.2) | 73(26.8) |
| COVID 19 can cause lung injury for those who recover | 174(64.0) | 98(36.0) |
| It is safe to see a COVID 19 patient with PPE | 235(86.4) | 37(13.6) |
| It is safe to operate on a COVID 19 patient without PPE | 58(21.3) | 214(78.7) |
| It is safe to live in the same house with a COVID 19 patient without maintaining physical distance | 27(9.9) | 245(90.1) |
| It is safe to stay in the same office with an asymptomatic COVID 19 patient with the AC on | 30(11.0) | 242(89.0) |
| There is no risk of infection if you see a COVID 19 patient in the same clinic with other patients | 55(20.2) | 217(79.8) |
| Disinfecting the clinics and waiting area with hydrogen peroxide reduces the chances of infection to zero | 132(48.5) | 140(51.5) |
| Wearing PPE’s (face mask, googles, gloves etc) will reduce the chances of infection among HCWs | 251(92.3) | 21(7.7) |
| Will you attend to a confirmed COVID 19 patient if provided with PPEs | 231(84.9) | 41(15.1) |
| Will you enter a ward where COVID 19 patients are kept if need be | 168(61.8) | 104(38.2) |
| Positive | Negative | Total | χ 2 | p value | |
| Variables | n (%) | n (%) | N (%) | ||
| Age | |||||
| 20 – 29 | 39 (95.1) | 2 (4.9) | 41 | 4.300F | 0.211 |
| 30 – 39 | 109 (92.4) | 9 (7.6) | 118 | ||
| 40 – 49 | 72 (88.9) | 9 (11.1) | 81 | ||
| 50 – 59 | 32 (100.0) | 0 (0.0) | 32 | ||
| Sex | |||||
| Male | 100 (92.6) | 8 (7.4) | 108 | 0.001 | 0.978 |
| Female | 152 (92.7) | 12 (7.3) | 164 | ||
| Educational qualification | |||||
| Secondary | 17 (81.0) | 4 (19.0) | 21 | 5.214F | 0.059 |
| Tertiary | 174 (92.6) | 14 (7.4) | 188 | ||
| Post tertiary | 61 (96.8) | 2 (3.2) | 63 | ||
| Marital status | |||||
| Single | 43 (97.7) | 1 (2.3) | 44 | 9.707F | 0.020* |
| Married | 205 (92.3) | 17 (7.7) | 222 | ||
| Divorced | 3 (100.0) | 0 (0.0) | 3 | ||
| Widow/ widower | 1 (33.3) | 2 (66.7) | 3 | ||
| Religion | |||||
| Christianity | 242 )92.4) | 20 (7.6) | 262 | 0.244F | 1.000 |
| Islam | 7 (100.0) | 0 (0.0) | 7 | ||
| Traditional | 3 (100.0) | 0 (0.0) | 3 | ||
| Tribe | |||||
| Yoruba | 229 (92.3) | 19 (7.7) | 248 | 0.392F | 1.000 |
| Others | 23 (95.8) | 1 (4.2) | 24 | ||
| Cadre | |||||
| Doctor | 73 (100.0) | 0 (0.0) | 73 | 17.488F | 0.003* |
| Nurses | 82 (93.2) | 6 (6.8) | 88 | ||
| Pharm | 5 (83.3) | 1 (16.7) | 6 | ||
| Lab | 14 (100.0) | 0 (0.0) | 14 | ||
| CHEW | 32 (88.9) | 4 (11.1) | 36 | ||
| Health attendants | 35 (85.4) | 6 (14.6) | 41 | ||
| Others | 11 (78.6) | 3 (21.4) | 14 | ||
| Years of practice | |||||
| < 5 years | 52 (89.7) | 6 (10.3) | 58 | 1.067F | 0.623 |
| 5 – 10 years | 76 (93.8) | 5 (6.2) | 81 | ||
| >10 years | 124 (93.2) | 9 (6.8) | 133 |
| Good | Poor | Total | χ 2 | p value | |
| Variables | n (%) | n (%) | N (%) | ||
| Age | |||||
| 20 – 29 | 37 (90.2) | 4 (9.8) | 41 | 1.294F | 0.754 |
| 30 – 39 | 103 (87.3) | 15 (12.7) | 118 | ||
| 40 – 49 | 74 (91.4) | 7 (8.6) | 81 | ||
| 50 – 59 | 30 (93.8) | 2 (6.3) | 32 | ||
| Sex | |||||
| Male | 103 (95.4) | 5 (4.6) | 108 | 6.224 | 0.013* |
| Female | 141 (86.0) | 23 (14.0) | 164 | ||
| Educational qualification | |||||
| Secondary | 19 (90.5) | 2 (9.5) | 21 | 4.715 | 0.095 |
| Tertiary | 164 (87.2) | 24 (12.8) | 188 | ||
| Post tertiary | 61 (96.8) | 2 (3.2) | 63 | ||
| Marital status | |||||
| Single | 42 (95.5) | 2 (4.5) | 44 | 2.049F | 0.580 |
| Married | 196 (88.3) | 26 (11.7) | 222 | ||
| Divorced | 3 (100.0) | 0 (0.0) | 3 | ||
| Widow/ widower | 3 (100.0) | 0 (0.0) | 3 | ||
| Religion | |||||
| Christianity | 234 (89.3) | 28 (10.7) | 262 | 0.293F | 1.000 |
| Islam | 7 (100.0) | 0 (0.0) | 7 | ||
| Traditional | 3 (100.0) | 0 (0.0) | 3 | ||
| Tribe | |||||
| Yoruba | 221 (89.1) | 27 (10.9) | 248 | 1.070F | 0.486 |
| Others | 23 (95.8) | 1 (4.2) | 24 | ||
| Cadre | |||||
| Doctor | 69 (94.5) | 4 (55.5) | 73 | 7.867F | 0.192 |
| Nurses | 76 (86.4) | 12 (13.6) | 88 | ||
| Pharm | 4 (66.7) | 2 (33.3) | 6 | ||
| Lab | 14 (100.0) | 0 (0.0) | 14 | ||
| CHEW | 31 (86.1) | 5 (13.9) | 36 | ||
| Health attendants | 37 (90.2) | 4 (9.8) | 41 | ||
| Others | 13 (92.9) | 1 (7.1) | 14 | ||
| Years of practice | |||||
| < 5 years | 56 (96.6) | 2 (3.4) | 58 | 9.466F | 0.009* |
| 5 – 10 years | 66 (81.5) | 15 (18.5) | 81 | ||
| >10 years | 122 (91.7) | 11 (8.3) | 133 |
| Good | Poor | Total | χ 2 | p value | |
| Variables | n (%) | n (%) | N (%) | ||
| Age | |||||
| 20 – 29 | 39 (95.1) | 2 (4.9) | 41 | 0.428F | 0.971 |
| 30 – 39 | 112 (94.9) | 6 (5.1) | 118 | ||
| 40 – 49 | 78 (96.3) | 3 (3.7) | 81 | ||
| 50 – 59 | 31 (96.9) | 1 (3.1) | 32 | ||
| Sex | |||||
| Male | 104 (96.3) | 4 (3.7) | 108 | 0.213F | 0.768 |
| Female | 156 (95.1) | 8 (4.9) | 164 | ||
| Educational qualification | |||||
| Secondary | 17 (81.0) | 4 (19.0) | 21 | 10.245F | 0.005 |
| Tertiary | 180 (95.7) | 8 (4.3) | 188 | ||
| Post tertiary | 63 (100.0) | 0 (0.0) | 63 | ||
| Marital status | |||||
| Single | 42 (95.5) | 2 (4.5) | 44 | 1.141F | 1.000 |
| Married | 212 (95.5) | 10 (4.5) | 222 | ||
| Divorced | 3 (100.0) | 0 (0.0) | 3 | ||
| Widow/ widower | 3 (100.0) | 0 (0.0) | 3 | ||
| Religion | |||||
| Christianity | 251 (95.8) | 11 (4.2) | 262 | 2.757F | 0.368 |
| Islam | 6 (85.7) | 1 (14.3) | 7 | ||
| Traditional | 3 (100.0) | 0 (0.0) | 3 | ||
| Tribe | |||||
| Yoruba | 237 (95.6) | 11 (4.4) | 248 | 0.004F | 1.000 |
| Others | 23 (95.8) | 1 (4.2) | 24 | ||
| Cadre | |||||
| Doctor | 71 (97.3) | 2 (2.7) | 73 | 7.300F | 0.200 |
| Nurses | 86 (97.7) | 2 (2.3) | 88 | ||
| Pharm | 6 (100.0) | 0 (0.0) | 6 | ||
| Lab | 12 (85.7) | 2 (14.3) | 14 | ||
| CHEW | 34 (94.4) | 2 (5.6) | 36 | ||
| Health attendants | 37 (90.2) | 4 (9.8) | 41 | ||
| Others | 14 (100.0) | 0 (0.0) | 14 | ||
| Years of practice | |||||
| < 5 years | 53 (91.4) | 5 (8.6) | 58 | 6.036F | 0.038 |
| 5 – 10 years | 76 (93.8) | 5 (6.2) | 81 | ||
| >10 years | 131 (98.5) | 2 (1.5) | 133 |
| Good | Poor | Total | χ 2 | p value | |
| Variables | n (%) | n (%) | N (%) | ||
|---|---|---|---|---|---|
| Knowledge | |||||
| Good | 236 (90.8) | 24 (9.2) | 260 | 7.216F | 0.025* |
| Poor | 8 (66.7) | 4 (33.3) | 12 | ||
| Attitude | |||||
| Positive | 225 (89.3) | 27 (10.7) | 252 | 0.655F | 0.704 |
| Negative | 19 (95.0) | 1 (5.0) | 20 |
Discussion
This study found that all the respondents have heard of COVID-19. This is not surprising considering that the study was carried out among HCW and also Covid 19 is a pandemic currently ravaging the world. Similar findings were also recorded in studies done in Nigeria, Uganda, China and other parts of the world 1, 5, 21, 22, 23, 24 Generally, majority 260 (95.6%) of the respondents in this study had good knowledge of Covid 19, this is also similar to findings in studies done in Nigeria15,21Greece,25 China23 and other parts of the world15,22,26,27
This study also found out that the most common source of information amongst the respondents on the disease was the internet/social media 187 (68.8%) followed by the Radio 94 (34.6%), this is in contrast to a study done in Greece24 and part of Nigeria 24 where the Radio was the most common source of information followed by the internet/social media. However, the findings were similar to those of studies done Nigeria and China 20,23 consequently, considering the importance of information dissemination to the control and eradication of Covid 19 stakeholders should use the internet/social media to disseminate information about Covid 19 more as this is a major source of information for HCWs. The traditional method of dissemination of information such as the radio and television should nonetheless not be discarded as this study also found that they are still a useful source of information dissemination.
Attitudes of people as a mediator between their knowledge and practices have an important role for better controlling of epidemics and pandemics of infectious diseases; they facilitate the process of changing people’s behaviour. Also, risk perceptions can influence health-related behaviours and change risky behaviours thus giving individuals a better outcome in the event of a health challenge.28 This study found that overall; the attitude of the majority of the HCWs was positive as evidenced by a total number of 252 (92.6%) HCWs with a positive attitude. This positive attitude may also be connected to the good knowledge exhibited by the respondents who are HCWs in this study. Similarly, this good knowledge was also associated with a high level of positive risk perception 244 (89/7%), similar findings were reported in studies done Nigeria 15Greece25 China29however, findings in this study contrasted sharply with findings in a study done in Iran where only about 50% of the respondents had a positive attitude towards Covid 1930. Study done by Srichan et al31 revealed that knowledge and attitudes 0toward disease prevention and control are poor in northern Tanzanian, while another study in Peru showed that over 75% of the respondents had a poor attitude to covid 1932. Ilesanmi et al in their study showed that there no significant difference existed in the risk perception, and KAP towards COVID-19 prevention among Doctors and Nurses 33. Most of the respondents in this study 236 (86.7%) agreed to follow the guidelines of the hospital Covid 19 taskforce this is in sharp contrast to findings in a study done in Thailand where only 15% of the respondents agreed to follow the Covid 19 guidelines
There is yet no cure for Covid 19 despite the extensive research on going on the diseases. The fact still remains that Covid 19 is a serious life threatening disease with a high mortality rate particularly in severe cases.1,4,5This study found that there was a high risk perception to covid 19, this may again be due to the fact that the sampling population were made up of HCWs. 244 (89.7%) of the respondents had a positive risk perceptionand this was similarto findings in another study done in Nigeria20
Limitations and Recommendations
This study is a hospital based study where the knowledge, attitude and risk perception is expected to be high due to the fact that the study population is made up of HCWs and as such can be used to use to assess the level of knowledge of health personnel which is expected to be higher than that of the community. This may also be a limitation, a community based study will help take care of this limitation, and similarly a comparative study between urban and rural communities will be more revealing. We recommend that similar study be conducted among different classes of people such as teachers, bankers, artisans, clergy etc
Conclusion
Overall, there was a high level of knowledge, high positive attitude and a high risk perception in the study. Consequently, to ensure that this high level is maintained, there is need for continuous health education and promotion.
Funding
This study was self funded
Ethical Approval
Ethical approval was sought and gotten from the Human Research and Ethical committee of the Federal Teaching hospital, Ido- Ekiti. Ekiti state
References
- 1. (2020) World Health Organization,Coronavirus Disease 2019(COVID-19): Situation Report, World HealthOrganization,Geneva. , Switzerland
- 2.Chan JFW, Kok K H, Zhu Z. (2020) Genomic characterization of the 2019 novel human-pathogenic coronavirusisolated from a patient with atypical pneumonia after visitingWuhan,”Emerging Microbes & Infections. 9(1), 221-236.
- 3.Yi Y, PNP Lagniton, Ye S, Li E, Xu R H. (2020) COVID-19: what has been learned and to be learned about the novel coronavirus disease. , Int J Biol Sci 16(10), 1753-1766.
- 4.Carod-Artal F J. (2020) Neurological complications of coronavirus and COVID-19. , Rev Neurol 70(9), 311-322.
- 6.Lai C C, Shih T P, Ko W C, Tang H J, Hsueh P R. (2020) Severe acute respiratory syndrome coronavirus 2(SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int JAntimicrob Agents. 55(3), 105924.
- 7.Guo Y R, Cao Q D, Hong Z S, Tan Y Y, Chen S D et al. (2020) The origin, transmission and clinicaltherapies on coronavirus disease 2019 (COVID-19)outbreak - an update on the status. Mil Med Res. 7(1), 11.
- 8.Labban L, Thallaj N, Labban A. (2020) Assessing the Level of Awareness and. , Knowledge of COVID 19 Pandemic among Syrians. ArchMed 12(2), 8.
- 14.Jekel J F, Katz D L, Elmore J G, Wild D. (2001) Sample size, randomization and probability theory. Epidemiology, Biostatistics and preventive medicine. , Philadelphia Saunders; 2, 194-199.
- 15.Olubunmi A, Aishat B U, Posi A, Abass G.Across-sectional study on Oyo State Health Care workers Knowledge, Attitude and Practice regarding Corona Virus Disease 2019(COVID-19).
- 16.Covid 19 Treatment guidelines Panel. Coronavirus disease 2019 (COVID-19) treatment Guidelines. National Institute of Health. Available athttps://www.covid19treatmentguidelines.nih.gov/.
- 17.National InterimGuidelines for Clinical Management of Covid 19. Nigeria Centre for Disease Control. Available at ncdc.gov.ng/covid19,ncdc.gov.ng. Accessed on 14/09/2020.
- 19. (2020) WHO DG’s opening remarks at the member state briefing on COVID-19. Available athttps://www.who.int/dg/speeches/details/whodirector general’s opening remarks at the member state briefing on covid-19….
- 20.Kanmodi K K, Nwafor N J, Amoo B A, Akinbami A A, Hundeji A A. (2020) Knowledge, risk perception, and attitudes of Nigerian dentists toward Covid-19: Pilot study. , Yen Med J 2(4), 30-37.
- 21.Zhong B L, Luo W, Li H M. (2020) Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID- 19 outbreak: a quick online cross-sectional survey. , Int J Biol Sci 16(10), 1745-1752.
- 22.Olum R, Chekwech G, Wekha G, Nassozi D R, Bongomin F. (2020) Coronavirus Disease-2019: Knowledge, Attitude, and Practices of Health Care Workers at Makerere University Teaching Hospitals, Uganda. Front Public Health. 8, 181.
- 23.Bhagavathula A S, Aldhaleei W A, Rahmani J, Mahabadi M A, Bandari D K. (2020) . Knowledge and Perceptions of COVID-19 Among Health Care Workers: Cross-Sectional Study. JMIR Public Health Surveill 6(2), 19160.
- 24.Fadeyi A, A O, MAN Adeboye, J A Awosanya, I O Oluwadiya et al. (2022) . , Knowledge, Attitude and Risk Perception of Covid-19 Among Nigerians. Fadeyi et al., Afr., J. Infect. Dis 16(2), 63-70.
- 25.Foteini M, Dimitrios G R, Ioanna V P. (2020) Assessment of Knowledge, Attitudes, and Practices towards New Coronavirus (SARS-CoV-2) of Health Care Professionals in Greece before the Outbreak Period. , Int. J. Environ. Res. Public Health 17, 4925.
- 26.Nwagbara U I, Osual E C, Chireshe R, Bolarinwa O A, Saeed B Q et al. (2021) Knowledge, attitude, perception, and preventative practices towards COVID-19 in sub-Saharan Africa: A scoping review. , PLoS ONE 16(4), 0249853.
- 27.Iheanacho T, Stefanovics E, Okoro U G. (2021) Assessing knowledge, attitude, practice and training related to COVID-19: a cross-sectional survey of frontline healthcare workers in Nigeria. , BMJ Open 11, 050138.
- 28.Behnam H, B L Kamran, Ali K, Fatemeh S, Mohammadhassan Z et al. (2020) Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: a population and field-based study from Iran. , International Journal of Public Health
- 29.Chen Y, Jin Y L, Zhu L J, Fang Z M, Wu N et al. (2020) The network investigation on knowledge, attitude and practice about Novel coronavirus pneumonia of the residents in Anhui Province Zhonghua yufang yi xue za zhi. Chinese journal of preventive medicine. 54(0), 4.
- 30.Behnam H, B L Kamran, Ali K, Fatemeh S, Mohammadhassan Z et al. (2020) Reza RH et al Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: a population and field-based study from Iran. , International Journal of Public Health
- 31.Srichan P, Apidechkul T, Tamornpark R, Yeemard F, Khunthason S. (2020) Knowledge, attitude and preparedness to respond to the 2019 novel coronavirus (COVID-19) among the bordered population of northern Thailand in the early period of the outbreak: a cross-sectional study. WHO South East Asia journal of public health. 992, 118-125.