
Risk Management: Emerging critical issues during the hospital administration of drug therapy
Abstract
Interruptions during pharmacological therapy in a hospital ward can be a source of error. We therefore considered two Operating Units of a hospital by asking the following questions: are the nursing staff who administer drug therapy at the set times able to do so with maximum concentration and without interruptions? If yes, how? If not, why and what for? Furthermore, are there organizational and non-organizational improvement strategies so that nurses are less interrupted during therapy and therefore do not cause adverse drug events that could cause harm to the patient? The results that emerged from the data analysis make us reflect considerably on how much interruptions during therapy are to be paid attention to as a problem to which solution proposals can be found.
Author Contributions
Academic Editor: ANUBHA BAJAJ, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2023 Lucio Mango, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Risk Management, or otherwise defined in the Healthcare sector, Clinical Risk Management, identifies the dangers and potential threats to which the hospital or in any case the healthcare company is subjected, defines and quantifies the hypothetical risk scenarios and formulates the most suitable countermeasures, pursuing strategic objectives well outlined 1.
The moment of pharmacological therapy represents the crucial phase of the therapeutic process, particularly in a hospital environment where there may be many critical issues emerging during its development. Often this activity is disturbed or even interrupted, as well as those who carry it out. Recent studies have shown a strong association between the rate of errors committed and staff interruptions 2.
Therefore it appeared useful to investigate through an experimental observational study on the moment of pharmacological therapy, to observe this moment, highlight the problems and try to propose strategies for improvement.
The present study aims to analyze some healthcare realities during the moment of pharmacological therapy, to observe if nurses get distracted during the performance of this important activity which appears to be a purely nursing responsibility and competence. Also, observe, when nurses get distracted, what are the main causes of interruptions; this because, as is well known, becoming aware of the cause of a problem is already the starting point for solving or reducing it. In this case, the qualitative increase in the care provided to those who use health services is obtained, with the hope of resolving and not worsening, as can often happen, health conditions.
It is known that, if human error cannot be completely eliminated, it is essential to work to obtain ideal working conditions and to implement a set of actions that make it difficult for man to make mistakes3.
We therefore considered two Operating Units of a hospital by asking the following questions: are the nursing staff who administer drug therapy at the set times able to do so with maximum concentration and without interruptions? If yes, how? If not, why and what for? Furthermore, are there organizational and non-organizational improvement strategies so that nurses are less interrupted during therapy and therefore do not cause adverse drug events that could cause harm to the patient?
Materials and Methods
The data were collected from two different types of operating units, the university Orthopedics and Traumatology and the university Emergency Medicine, respectively.
Starting from June and until September 2018, in both hospitalizations, questionnaires were administered, with consent, to the caregivers of the patients and to the nurses, to have a vision of their conception of the moment of drug therapy and the importance that both caregivers and nurses attribute to the latter. The questionnaire (appendix, attachment 1-2) is the same for nurses and caregivers, apart from one more question present in the questionnaire addressed to nurses, and consists of 11/12 questions. It can ideally be divided into four areas. The first part concerns the sampling of the study: the operating unit in which the questionnaire is being filled in, i.e. whether it concerns the surgical or medical area, and some of the personal data of the person completing it, including age, gender , educational qualification and working years, all in compliance with privacy regulations. The second part, which includes the first three questions, served to get to know the idea that nurses and caregivers have of therapy, how they see this moment and how much importance they attribute to it, even with respect to the medical visit. The third part, which instead includes questions from fourth to sixth (or seventh in the case of nurse questionnaires) concerns the problem of possible distractions of the nurse during therapy; in fact, those who fill out the questionnaire are asked if they have been able to ascertain that this moment is often disturbed, how much, for what causes and if the continuous interruptions can lead to a clinical risk for the patient. In the case of the questionnaires addressed to nurses, the additional question, the seventh, asks them to explain what type of errors or near misses they have encountered due to the interruptions. The last part however, which goes from question 8/7 (depending on whether it is the questionnaire addressed to the family members of the patients or to the nurses) to the last, as well as assessing the presence of a family member or caregiver during the therapy, aims more to know the possible "solutions" to be implemented to avoid distractions during drug therapy. For this reason, it is asked whether it could be useful, for example, to keep relatives or caregivers away from the division during the moment of therapy, or to provide the patient with clarifications, prior to administration, to explain and reassure him about what is about to be administered.
Results
In total, a total of nineteen completed by nurses and forty-six completed by caregivers questionnaires were obtained. The data analysis is reported in the form of graphs performed with the EXCEL 2013 program.
The graphs of question number 3 of both questionnaires (that it is nothing more than the motivation for the answer to question 2), of question number 7 of the nurses questionnaire (which asks what types of errors they encountered due to interruptions) and of the question "How, in your opinion, could the nurse who administers the therapy be prevented from being interrupted and distracted?" of both questionnaires, were not done as they required a discursive response.
The table of data concerning the characteristics of the interviewees and the graphs of the answers to the various questions then follow: Table 1
Table 1. Sampling| CAREGIVER | NURSES | |
| SEX | ||
| Male | 48% | 26.32% |
| Female | 52% | 73.68% |
| AVERAGE AGE | 50 years old | 35 years old |
| DEGREE | ||
| middle School | 28.3% | 0% |
| high school diploma | 45.65% | 15.78% |
| bachelor's degree | 6.52% | 84.22% |
| master's degree | 19.53% | 0% |
| WORKING YEARS | ||
| 1-4 | 6.52% | 36.9% |
| 5-10 | 13% | 26.3% |
| 11-20 | 17.48% | 26.3% |
| more than 20 | 63% | 10.5% |
This graph shows that only 10% of the caregiver population consider therapy as a mere administration of drugs. Instead, all the nurses and about 90% of the rest of the caregivers seem to agree that therapy is something a little more complex than a simple administration of drugs. graph 1
Graph 1.What is therapy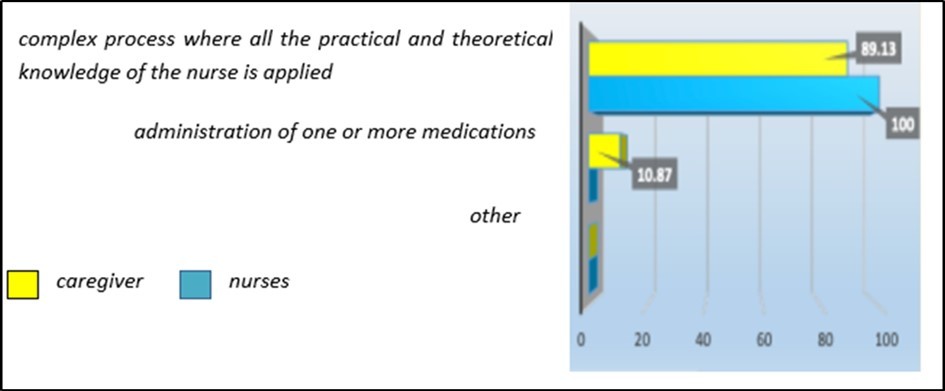
It seems that only 2% of family members consider therapy less important than a medical visit, while the rest, i.e. most of them, attribute the same importance to it as a medical visit, as do just over half of the nurses. graph 2
Graph 2.What importance do you give to therapy?
This graph shows quite conflicting results between nurses and caregivers. In fact, approximately 63% of nurses declare that they feel "very" interrupted, while 52.17% of family members seem to be convinced that the nursing staff is "little" interrupted during therapy. graph 4
Graph 4.How much do you think the nurse is interrupted during therapy?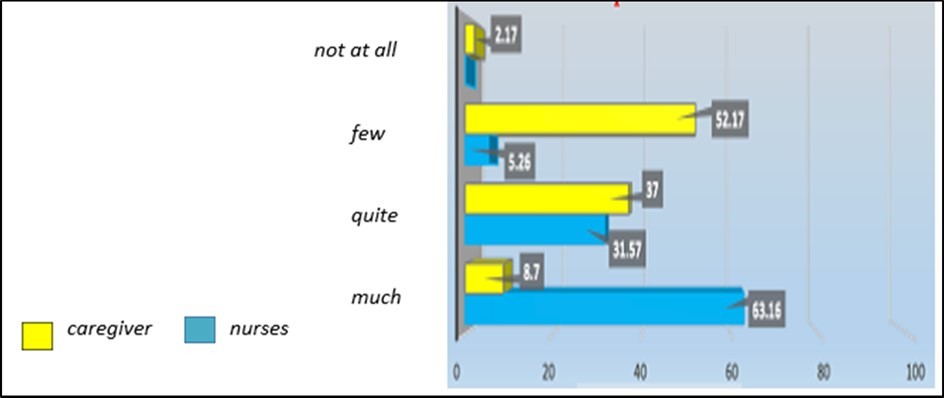
As can be seen from this graph, nursing staff and caregivers have opinions that sometimes converge and sometimes differ on what, according to them, are the main causes that lead nurses to distraction. More than 50% of nurses declare that it is the patient's bells, the ward intercom, family members and colleagues that cause most of their distractions during the moment of therapy, while only 47.82% of family members or patient caregivers think they be themselves a cause of nurse interruptions. On the other hand, nurses and caregivers seem to agree on distractions due to patient needs. In addition, nearly 50% of nurses feel distracted by the fact that they often have to step away from the therapy cart to ask the doctor about incomplete or incorrect prescriptions. graph 5
Graph 5.What are the main causes of distraction?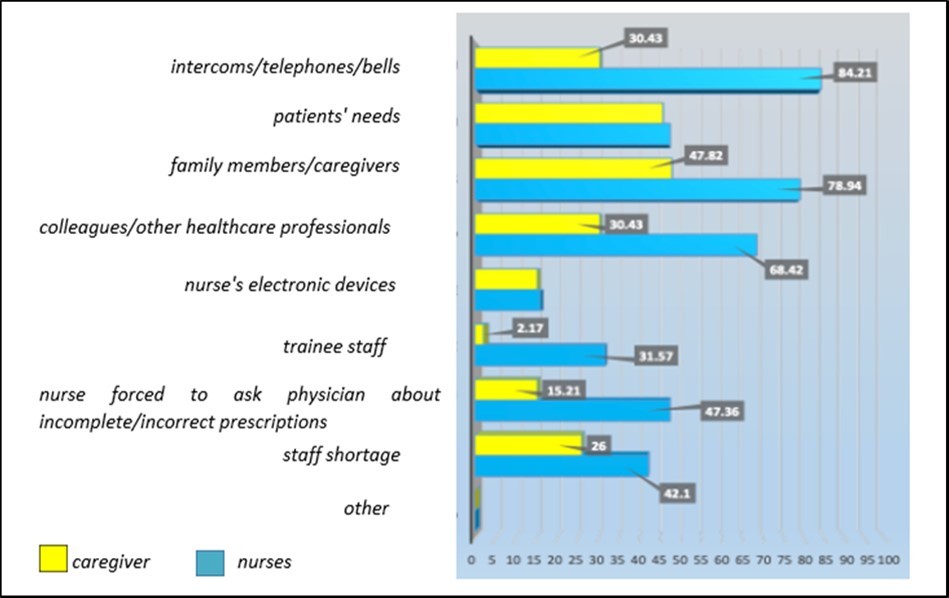
The results of the graph show how almost 70% of nurses are aware of the fact that interruptions during therapy "significantly" increase the risk of error and also the opinion of family members seems to find this confirmation, because just over half of them stated that interruptions have a “fairly” negative impact on the patient. Unfortunately, a part of caregivers, even if small (4%), declares that interruptions during therapy do not increase the risk of errors and therefore of adverse drug events "at all". graph 6
Graph 6.How much do distractions during therapy increase the risk of error?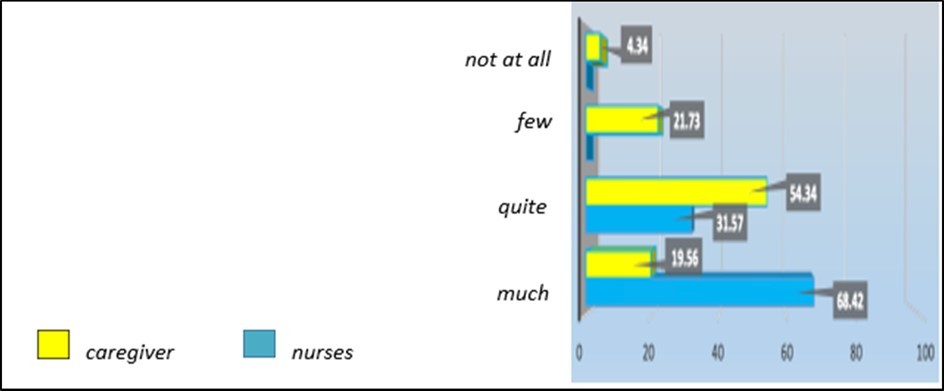
This graph provides us with information on how the presence of caregivers or family members can influence the moment of therapy. The opinion of nurses (52%) and caregivers (45, 65%) appears to be similar regarding regarding relatives as a source of distraction. However, about 30% of the nursing staff declare that the family member can help them in preventing any errors in therapy. Only 21% of caregivers think that family members themselves can act as input for the nurse so that the latter does his best. graph 7/8
Graph 7/8.How do you evaluate the presence of a family member/caregiver during the therapy?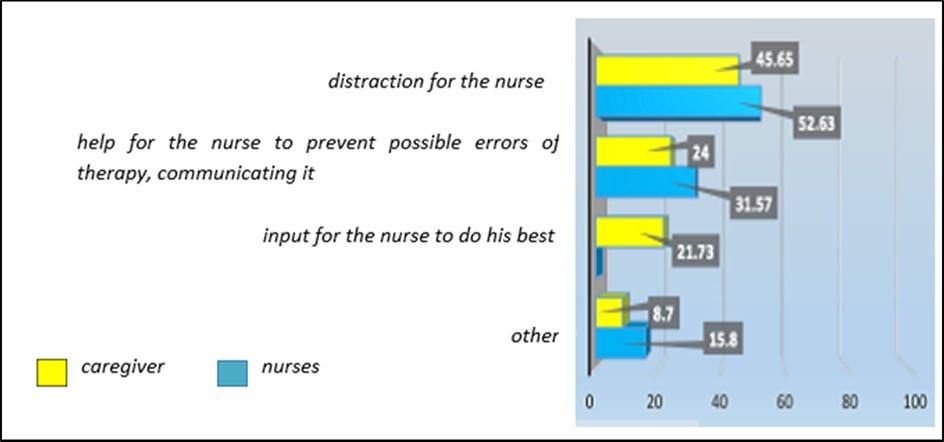
The results of this question, addressed to both nurses and caregivers, show fairly unanimous opinions on the fact that providing information to the patient or caregiver on the therapy that is about to be administered could prevent the family member from interrupting the nurse for clarification or reassurance about therapy. Oddly, 31% of nurses think that providing clarification will not help reduce interruptions. graph 8/9
Graph 8/9.Can providing clarifications on the therapy to be administered reduce doubts and therefore interruptions?
This graph shows that almost 80% of nurses agree that therapy, especially infusion therapy, could be prepared in a protected area, which could be the infirmary or in any case an area where there is a greater flow of people. graph 9/10
Graph 9/10.Do you think preparing medications in a "protected area" could avoid nurse interruptions?
Discussion
In the light of the results obtained, it is certainly very clear that the nurse is rarely able to start and conclude the moment of drug therapy without ever being interrupted. The causes of the occurrence of the interruptions are certainly multifactorial. In fact, from what emerges from both the opinion of nurses and caregivers, the majority of interruptions are due to the following main reasons:
Fellow nurses or healthcare personnel in general. (a colleague to ask about other patients; a doctor who needs to add/modify something to a patient's therapy; ambulance workers who ask for a specific patient to be transferred)
Relatives or caregivers of the patients. From the objective observation of the various moments of the therapy, it can be seen that family members or caregivers, both in the medical and surgical areas, represent one of the most frequent sources of interruptions (about 75%). In support of this information are the results of the graph with reference to question 7/8, in which even 53% of the nurses maintain that the family members of the patients represent a source of distraction. It makes us think that some family members, despite knowing the importance of the moment of therapy and having justified their response (question 3 of the questionnaire) by saying that, unlike a medical visit, "if you make a mistake in giving a tablet, you can never go back ”, they persevere in a conduct that does not favor a climate of safety and concentration for those who are committed to carrying out drug therapy in the best possible way, whose mistakes could compromise the health of their own loved ones.
Restore equipment, supplies or drugs missing from the drug therapy trolley, a problem that causes the nurse to leave the therapy trolley frequently.
Check alarms (intercom, telephone, patient bells, infusion pump alarms). Trivially, among the organizational dysfunctions that lead to interruptions we find the continuous sounds of alarms such as intercoms, telephones, bells, etc. The adverb "trivially" has not been used to indicate a problem that assumes less importance than the others, but because it seems to be a fairly solvable question if all the professional figures that revolve around the patient contribute to facilitating the nurse during therapy. In fact, he often finds himself literally bombarded by the various "sounds of the division" which do not favor his concentration and which consequently increase the probability of adverse drug events.
Patient needs. This cause of distraction can be less remedied, since most of the needs of patients, other than the doctors, can only be attended to by healthcare professionals and nurses. Particularly, the significant number of interruptions due to the needs of patients prevails in the medical area(87.5%) rather than in the surgical area (55.5%).This can probably be explained by the fact that the more critical patients' clinical conditions, usually characteristic of critical area of medical departments, require more nursing support. Often patients interrupt to express doubts about the therapy that they are about to be administered. This is precisely the reason why the question of what they think about the possibility of providing clarifications on what is being administered to them was included in the questionnaire. The results of the answers to this question showed that 87% of family members/caregivers believe that providing information to the patient or whoever assists him on what concerns the therapy he must take would reduce interruptions; 68% of nurses also agree with this idea.
Trainees within the hospital, such as undergraduate nursing students and medical residents. Among the declarations of the nurses (see graph question 5) it emerges that the interruptions due to this cause cover the high percentage of 68%.
Although 42% of nurses believe that another major cause of nursing interruptions is understaffing (see chart question 5), objective observation does not reveal meaningful evidence for these findings. The problem of staff shortage is well known, but this does not significantly affect the problems related to the interruption of therapy, but rather to problems of an organizational nature and psychophysical stress affecting the nursing staff.
Finally, as regards the consequences of interruptions, in the nurses' questionnaire there is an additional question, which, as mentioned above, is number 7. In it, they are asked to describe what types of errors they have experienced due to interruptions in therapy. From what was answered, it emerged that the problem of interruptions during preparation and/or administration does not lead to skill-based errors, but it is, more than anything else, a problem that does not allow the nurse to concentrate on the therapy and carry out all the evaluations and reasoning necessary before administering even just one tablet. Therefore, the distractions faced by the nurse represent the typical situation that also leads to the famous planning errors (mistakes)4. Nurses reported that the most common types of errors or near misses were dosing, identification, and preparation.
Conclusion
The results that emerged from the data analysis make us reflect considerably on how much interruptions during therapy are to be paid attention to as a problem to which solution proposals can be found. All this for the sole purpose of protecting the well-being of the patients, given that according to the literature, as the occurrence of nursing interruptions increases, the probability of incorrect administrations increases by 60%. Furthermore, according to Canadian studies of 2010 5, 6 interruptions lead to a 12% increase in errors in therapy.
Although a variety of interventions have been introduced into the healthcare system, these interventions have rarely been sustainably used in hospitals 7.
It has been said here that one cause of interruption is represented by family members and colleagues; there could be three possible solutions to try to contain this phenomenon.
One of these is of an educational nature and involves the creation of a brochure to be delivered to each assisted person who becomes part of an operating unit, be it a long-term or short-term stay. In this brochure it would be appropriate to include all the negative consequences that interruptions aimed at the nurse during drug therapy could lead to. In this way, patients could understand the need not to interrupt the nurse engaged in therapy, for the sake of their own health, and not for a refusal of the nursing staff to communicate. Probably in this way the patient would be more willing and cooperative towards the nursing staff, provided that he/she witnesses an availability of help and possible clarifications towards him/her from the nurses. The same brochure could be affixed to each hospital room so that the message also reaches all visitors.
To reduce interruptions during the administration of therapy, in recent years some English hospitals have been introduced in colored jackets with the words "I am preparing the therapy, do not interrupt". This method of preventing or, at least, reducing interruptions during the administration of drug therapy has actually seen and sees some contradictions.
We have seen that there are some avoidable interruptions, intrusive interruptions, and others that are inevitable, i.e. necessary for carrying out the care activity, and therefore identifiable as cooperative interruptions 8, namely interruptions that help, and others that hinder a work process or a interaction. Nurses wearing “Do Not Disturb” jackets are less approachable, or so they appear to patients and family members or caregivers. This can result in a feeling of negativity, given the role and trust that are associated with the figure of the nurse, although in any case the jackets seem to have a potential positive effect because they reduce interruptions and, in this way, help to buy time dedicated to patients. It can be concluded that the evidence in favor of jackets still appears limited 10, much more experiences and evaluations will probably be needed, perhaps through questionnaires, to better judge their validity.
Technology is definitely a way to cut down or greatly reduce all adverse drug events related to misidentification, dosage, etc. 11. In some healthcare realities the electronic bracelet has already been adopted, in others the computerized folder, in still others the so-called "smart trolley" 12. This technical device guides the nurse in loading the trolley itself with the drugs needed for administration, automatically recognizes the room it is in and automatically recognizes the opening of a drawer, continuing to guide the nurse in finding the right drug, also signaling the possible opening of a wrong drawer 13.
Finally, it is certain that improvements can be obtained through an appropriate organization, accompanied by training sessions, both for health professionals and for family members and caregivers 14.
References
- 1.Mango L. (2021) Le aziende sanitarie e la “Clinical Governance”. Edizioni Mediche Scientifiche Internazionali (EMSI). , Roma
- 2.A J Spooner, Corley A, Chaboyer W. (2015) Measurement of the frequency and source of interruptions occurring during bedside nursing handover in the intensive care unit an obser vational study Australian Critical Care. 28(1), 19-23.
- 3.Reason J. (1990) Human error. Cambridge university press.Edizione italiana: L’errore umano. Il Mulino Editore. , Bologna
- 4.Nadj M, Maedche A, Schieder C. (2020) The effect of interactive analytical dashboard features on situation awareness and task performance. Decision support systems. 135, 113322.
- 5.McGillis Hall L, Pedersen C, Hubley P. (2010) Interruptions and pediatric patient safety. , J Pediatr Nurs 25, 167-75.
- 6.J I Westbrook, Woods A.Rob M.I..(2010 Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med;170:. 683-90.
- 7.Sadeghi M, Sasangohar F. (2018) Investigating nursing task interruptions in intensive care units: A scoping literature review. In 62nd Human Factors and Ergonomics Society Annual Meeting. HFES 478-479.
- 9.Ferro M, Vecchiato S, Pascolo M. (2014) Il dibattito sulle casacche segnaletiche per prevenire le interruzioni durante il giro della terapia: una revisione narrativa. , L’infermiere 51, 23-29.
- 10.Berdot S.Vilfaillot A.,Bezie Y.(2021) Effectiveness of a ‘do not interrupt’ vest intervention to reduce medication errors during medication administration: a multicenter cluster randomized controlled trial. , BMC Nurs; 20, 153.
- 11.Yeasmin S. (2019) Benefits of artificial intelligence in medicine. In 2019 2nd International Conference on Computer Applications & Information Security. (ICCAIS) 1-6.